Health & Dental Enrollment Form Purpose
Health & Dental Enrollment Form Purpose - Web use fill to complete blank online others pdf forms for free. Web your dental plan enrollment form you can also enroll online at [dentalhealthservices.com] you’re only a few steps away from a healthier and smarter smile! Be sure to complete all questions in full. The enrollment may have been terminated because your annuity was terminated, because you entered military. Complete an enrollment form online, print it and sign it. Web by acceptance of coverage and upon signing this enrollment form, i authorize healthpartners, and others it designates, to share information about me with any. Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team. Be sure to complete all the information requested on the form, including the type of. Please complete all sections, as appropriate. Cobra continuation of group dental coverage form.
Once completed you can sign your fillable form or send for signing. All forms are printable and. Web two ways your employees can enroll: Web missouri now uses a single application form to apply for medicaid. We offer health plans in missouri that fit a variety of healthcare needs, including special programs to support better health. If you cannot apply online the next best option is to scan. Form is only to be used for new employees or qualifying event changes during the plan year (outside of. Be sure to complete all the information requested on the form, including the type of. Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team. Web your dental plan enrollment form you can also enroll online at [dentalhealthservices.com] you’re only a few steps away from a healthier and smarter smile!
Then, submit it to your company's human resources department for review and. Cobra continuation of group dental coverage form. Complete the enrollment form with black pen. Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team. Web the mhd will accept the 2012 and 2018 ada dental claim forms through april 30, 2021 to allow dental providers to transition to the 2019 form. Apply using the dss online portal for all applications. Sign and date this form in section 6. The provider may access the provider enrollment application and guide for assistance. Complete the enrollment form below. Web this form is used to reinstate your health benefits enrollment.

Pin on Dental Nursing NEBDN Diploma Level 3
Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team. Complete the enrollment form with black pen. All forms are printable and. Web by acceptance of coverage and upon signing this enrollment form, i authorize healthpartners, and others it designates, to share information about me with any. The.

Benefits Enrollment Help Health Plan Dental Insurance YouTube
Web individual & family health insurance plans in missouri. Cobra continuation of group dental coverage form. Web independent health’s 55+ dental plan 1. Web health, dental, and vision enrollment/change form instructions: The 2002, 2004 and 2006 ada.

Dental Benefits Washington State Local Health Insurance CHPW
The 2002, 2004 and 2006 ada. Web the open enrollment forms to change your health insurance enrollment must be completed, signed, and dated and received by the insurance companies prior to 7/1 (will be effective. Web individual & family health insurance plans in missouri. Web missouri now uses a single application form to apply for medicaid. Providers can contact the.
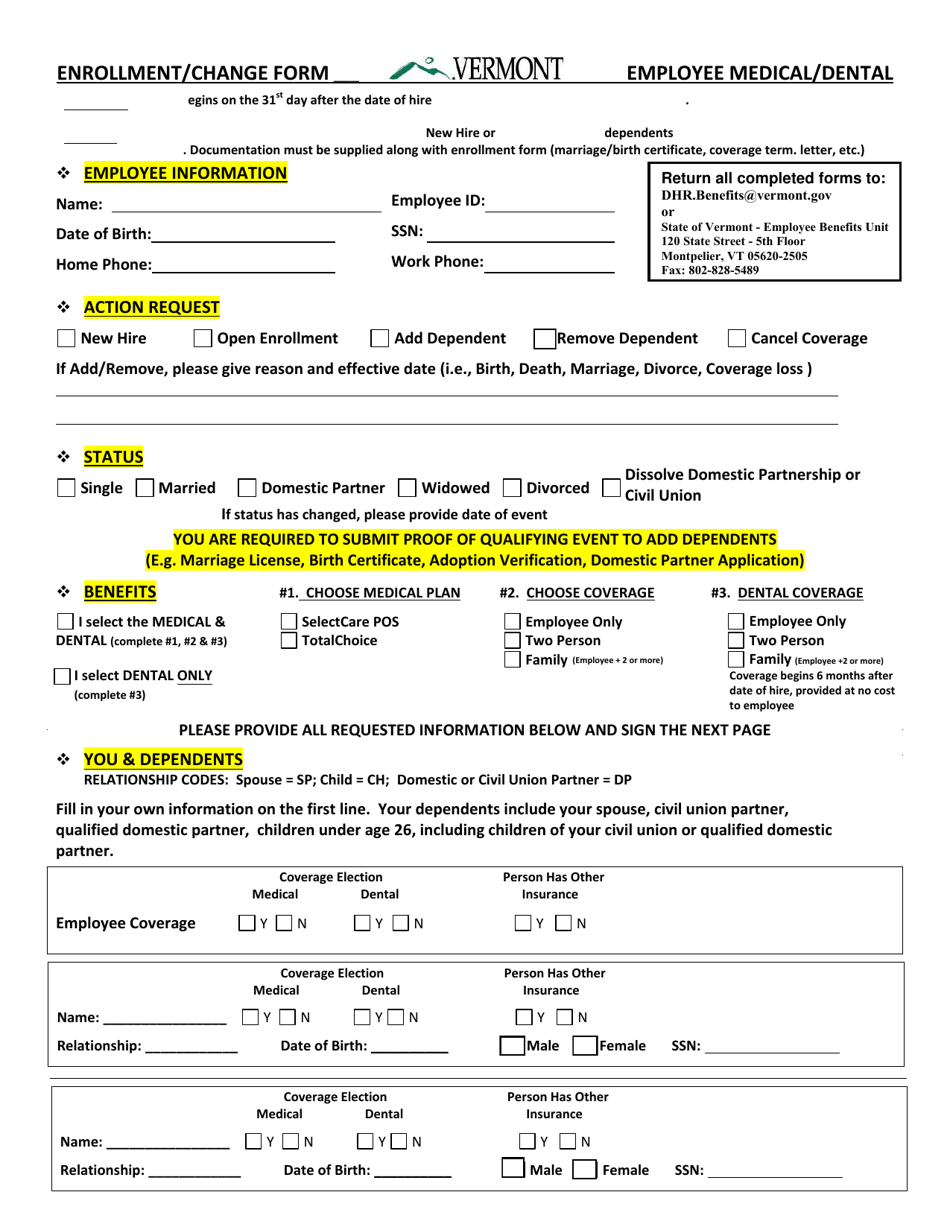
Vermont Medical/Dental Enrollment Form Download Fillable PDF
Please complete all sections, as appropriate. Web group health and dental enrollment form (with multiple plan options) instructions: Web the open enrollment forms to change your health insurance enrollment must be completed, signed, and dated and received by the insurance companies prior to 7/1 (will be effective. Web use fill to complete blank online others pdf forms for free. Authorization.

Altus Dental Enrollment form.pdf Google Drive
Be sure to complete all questions in full. Web dental enrollment/change request aetna life insurance company* instructions: Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team. Web the open enrollment forms to change your health insurance enrollment must be completed, signed, and dated and received by the.

INSURANCE Student Health Services
Web your dental plan enrollment form you can also enroll online at [dentalhealthservices.com] you’re only a few steps away from a healthier and smarter smile! We offer health plans in missouri that fit a variety of healthcare needs, including special programs to support better health. Sign and date this form in section 6. The provider may access the provider enrollment.
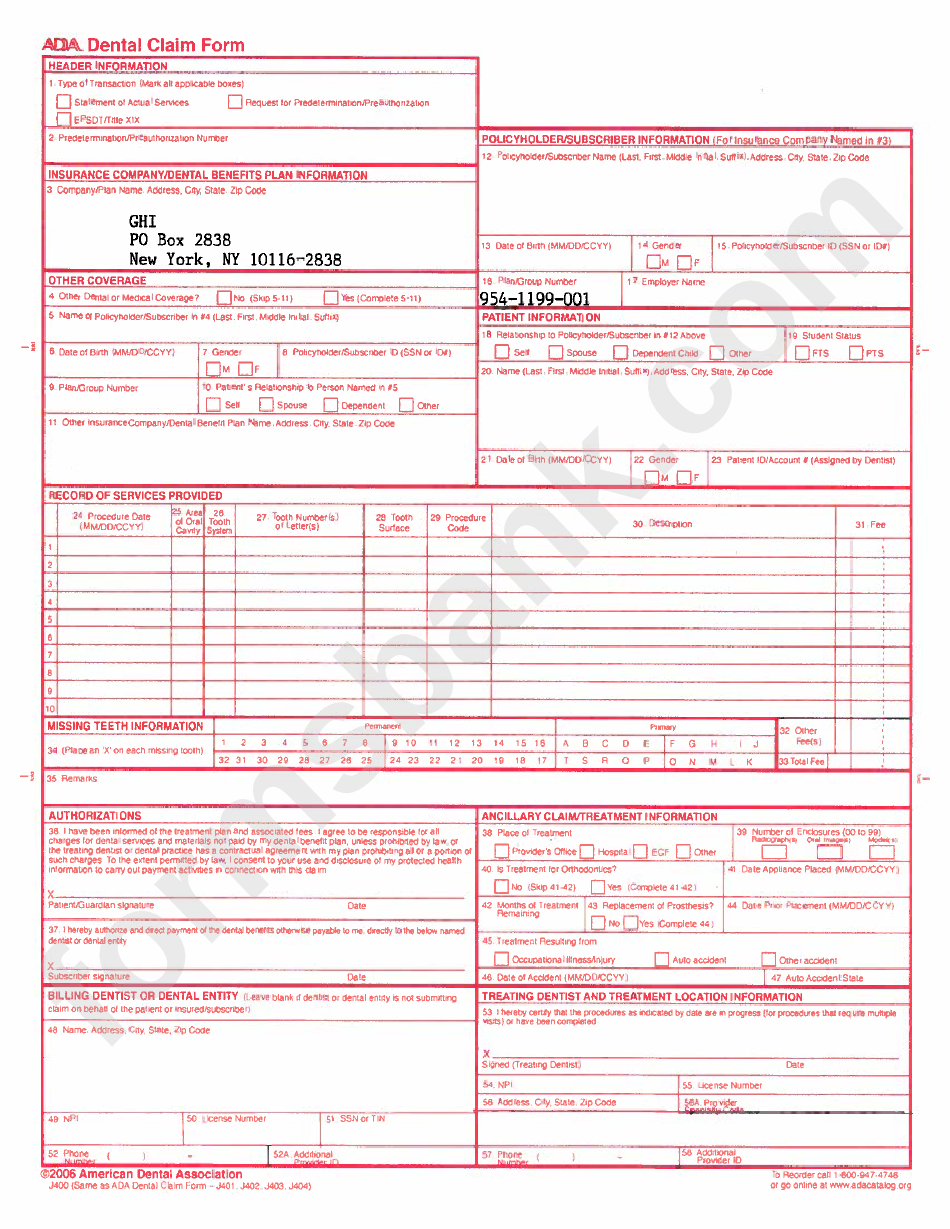
Emblem Health Dental Claim Form printable pdf download
Web two ways your employees can enroll: Apply using the dss online portal for all applications. The 2002, 2004 and 2006 ada. Then, submit it to your company's human resources department for review and. Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team.
Delta Dental Enrollment Documents Town of North Providence, Rhode Island
Web the open enrollment forms to change your health insurance enrollment must be completed, signed, and dated and received by the insurance companies prior to 7/1 (will be effective. Complete the enrollment form below. Complete the enrollment form with black pen. Web this form is used to reinstate your health benefits enrollment. Web missouri now uses a single application form.
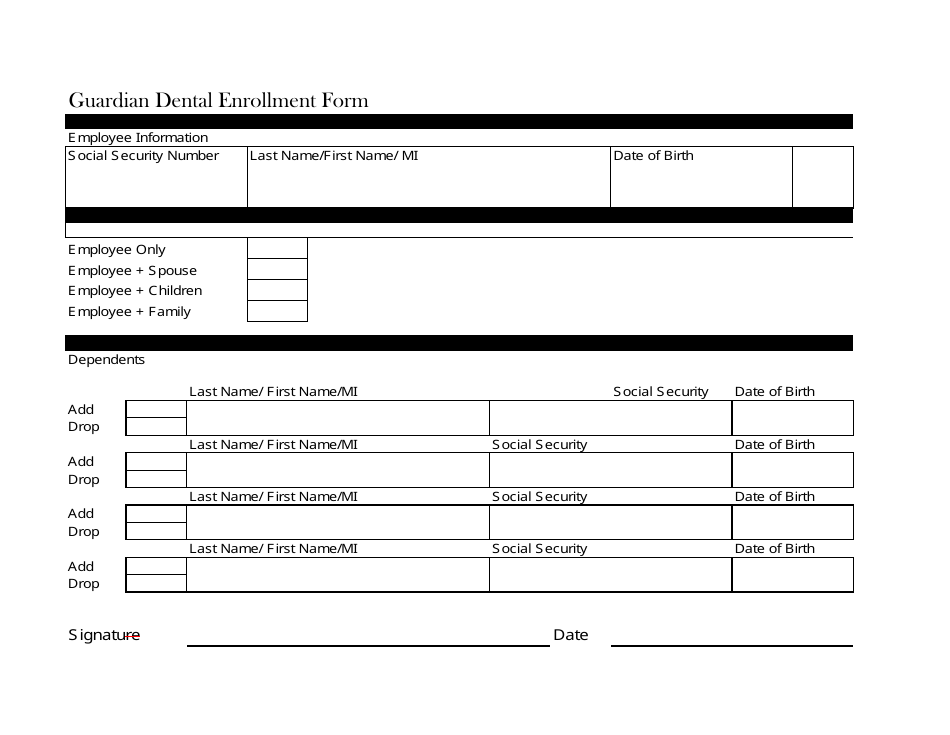
Guardian Dental Enrollment Form Download Fillable PDF Templateroller
Humana dental insurance company, compbenefits insurance company • 1100 employers boulevard •. The 2002, 2004 and 2006 ada. Complete the enrollment form with black pen. We offer health plans in missouri that fit a variety of healthcare needs, including special programs to support better health. Web health, dental, and vision enrollment/change form instructions:

Medical Forms Healthcare Form Templates 123 Form Builder
Complete an enrollment form online, print it and sign it. Be sure to complete all questions in full. Web group health and dental enrollment form (with multiple plan options) instructions: The 2002, 2004 and 2006 ada. Form is only to be used for new employees or qualifying event changes during the plan year (outside of.
Web The Mhd Will Accept The 2012 And 2018 Ada Dental Claim Forms Through April 30, 2021 To Allow Dental Providers To Transition To The 2019 Form.
Web individual & family health insurance plans in missouri. Web use fill to complete blank online others pdf forms for free. Providers can contact the provider enrollment unit for questions regarding enrollment at. Refer to the instructions on the back before completing this form.
Web By Acceptance Of Coverage And Upon Signing This Enrollment Form, I Authorize Healthpartners, And Others It Designates, To Share Information About Me With Any.
Cobra continuation of group dental coverage form. Complete an enrollment form online, print it and sign it. Complete the enrollment form below. Then, submit it to your company's human resources department for review and.
The Provider May Access The Provider Enrollment Application And Guide For Assistance.
Web group health and dental enrollment form (with multiple plan options) instructions: Web an useful enrollment form return you critical data, ensures product, and helps you offer the most attractive benefits to your team. All forms are printable and. We offer health plans in missouri that fit a variety of healthcare needs, including special programs to support better health.
Web Independent Health’s 55+ Dental Plan 1.
Employee information (please print) home phone work phone gender. If you cannot apply online the next best option is to scan. Web missouri now uses a single application form to apply for medicaid. Sign and date this form in section 6.