Cms-1500 Claim Form Instructions
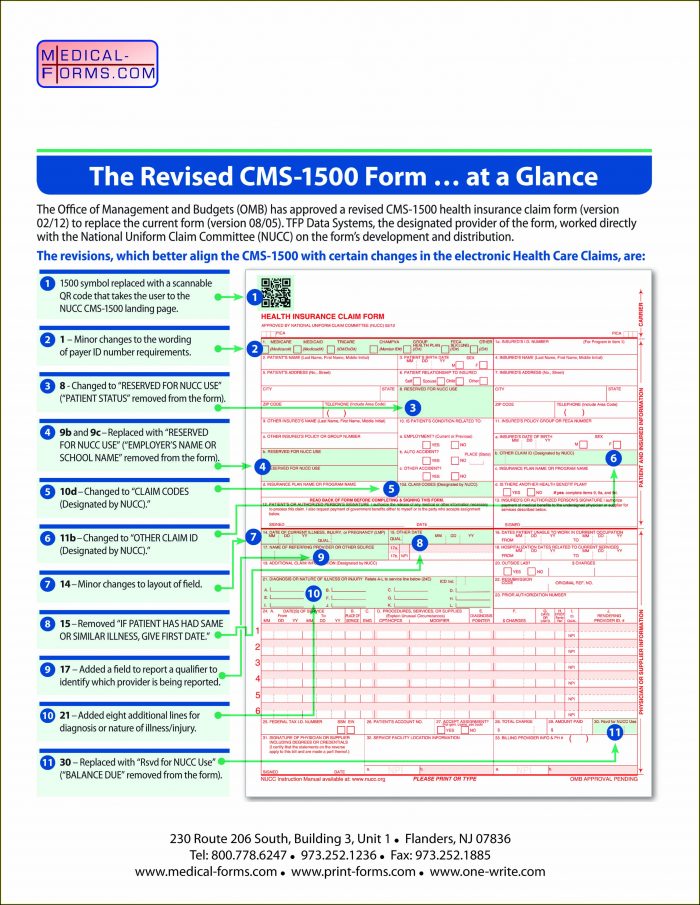
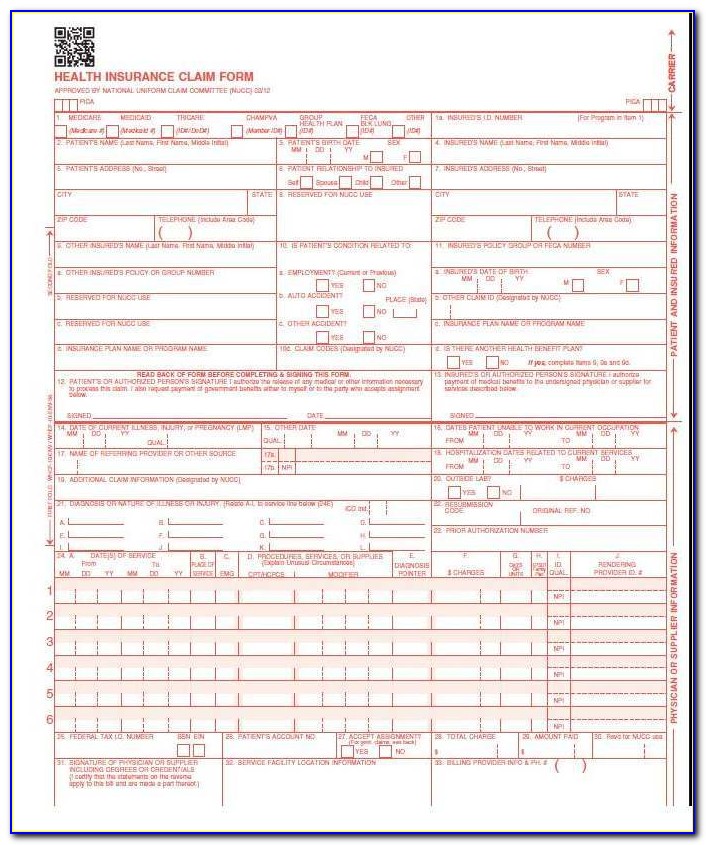
Cms-1500 Claim Form Instructions - Number (for program in item 1) 4. Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. Web cms 1500 claim form instructions tool. Form version 02/12 will replace the current cms 1500 claim form, 08/05, effective with claims. Web cms 1500 dynamic list information. To view instructions, hover over each field. For complete instructions, refer to chapter 6 of the dme supplier manual. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or. Web revised cms 1500 claim form, version 02/12. State the type of health insurance applicable to.
For complete instructions, refer to chapter 6 of the dme supplier manual. The form is used by physicians and allied health professionals to. Fill out the health insurance claim form online and print it out for free. Ad access any form you need. In order to increase health care provider participation in the workers' compensation system and improve injured workers' access to timely, quality medical. To view instructions, hover over each field. Web cms 1500 (02/12) claim form instructions cms 1500 (02/12) claim form instructions note: Insured’s name (last name, first name, middle initial). This form is the only version. Complete, edit or print your forms instantly.
Web cms 1500 dynamic list information. Web you, your employees and agents are authorized to use cpt only as contained in the following authorized materials including but not limited to cgs fee schedules, general. To view instructions, hover over each field. State the type of health insurance applicable to. Web cms 1500 (02/12) claim form instructions cms 1500 (02/12) claim form instructions note: Form version 02/12 will replace the current cms 1500 claim form, 08/05, effective with claims. Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare replacement plan” in the left top. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or. Number (for program in item 1) 4. Fill out the health insurance claim form online and print it out for free.
Cms 1500 Claim Form Instructions 2016 Form Resume Examples XE8je6e3Oo
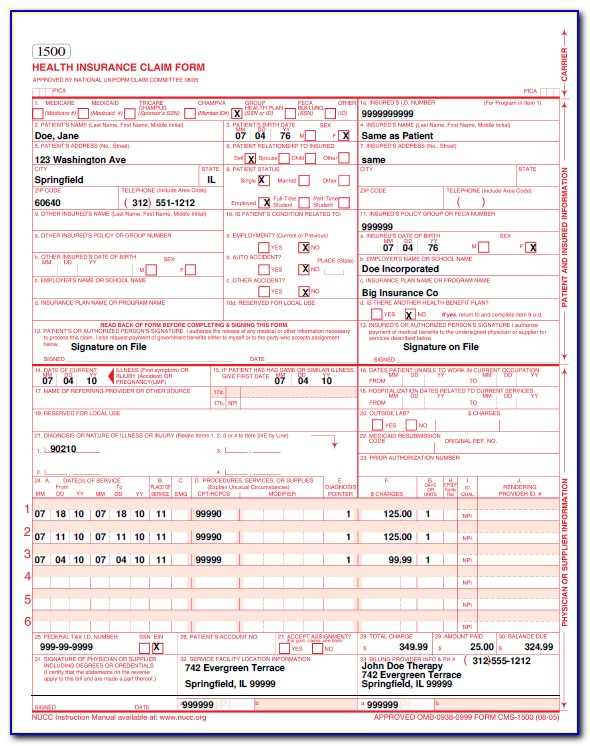
Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. For complete instructions, refer to chapter 6 of the dme supplier manual. This form is the only version. Insured’s name (last name, first name, middle initial). Web item 1 item 1a item 2 item 3 instructions type of health insurance.

Cms 1500 Claim Form Instructions Pdf Universal Network
Web cms 1500 claim form instructions tool. The form is used by physicians and allied health professionals to. Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. Ad access any form you need. Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare.

Medicare Form 1500 Instructions Form Resume Examples QJ9el08B2m
Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. Web item 1 item 1a item 2 item 3 instructions type of health insurance coverage applicable to the claim show the type of health insurance coverage applicable to this claim by. Insured’s name (last name, first name, middle initial). Web.

Cms 1500 Claim Form Instructions 2016 Form Resume Examples XE8je6e3Oo
Form version 02/12 will replace the current cms 1500 claim form, 08/05, effective with claims. Web revised cms 1500 claim form, version 02/12. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or. Web cms 1500 (02/12) claim form instructions cms 1500 (02/12) claim form instructions note: Web cms 1500 claim form instructions.

Cms 1500 Form Instructions 2018 Universal Network
In order to increase health care provider participation in the workers' compensation system and improve injured workers' access to timely, quality medical. Web cms 1500 dynamic list information. Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for medical services. Form version 02/12 will replace the current cms 1500 claim form, 08/05,.
Cms 1500 Claim Form Instructions Workers Compensation Form Resume
Web cms 1500 claim form instructions tool. To view instructions, hover over each field. Web how to submit claims: Web cms 1500 (02/12) claim form instructions cms 1500 (02/12) claim form instructions note: For complete instructions, refer to chapter 6 of the dme supplier manual.

SAMPLE CMS 1500 form CMS 1500 claim form and UB 04 form
Ad access any form you need. Insured’s name (last name, first name, middle initial). The form is used by physicians and allied health professionals to. State the type of health insurance applicable to. This form is the only version.

Cms 1500 Form 212 Instructions Universal Network
Number (for program in item 1) 4. Web cms 1500 (02/12) claim form instructions cms 1500 (02/12) claim form instructions note: Complete, edit or print your forms instantly. For complete instructions, refer to chapter 6 of the dme supplier manual. The form is used by physicians and allied health professionals to.

Cms 1500 Claim Form Pdf Free Download Universal Network
Web revised cms 1500 claim form, version 02/12. State the type of health insurance applicable to. Ad access any form you need. To view instructions, hover over each field. Complete, edit or print your forms instantly.
Cms 1500 Claim Form Instructions Workers Compensation Form Resume
Form version 02/12 will replace the current cms 1500 claim form, 08/05, effective with claims. Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare replacement plan” in the left top. Web how to submit claims: Web the center of medicaid and medicare services (cms) form 1500 must be used to bill sfhp for.
Web The Center Of Medicaid And Medicare Services (Cms) Form 1500 Must Be Used To Bill Sfhp For Medical Services.
Description and instructions n/a situational when submitting a medicare replacement plan claim, write or stamp “medicare replacement plan” in the left top. Number (for program in item 1) 4. Web you, your employees and agents are authorized to use cpt only as contained in the following authorized materials including but not limited to cgs fee schedules, general. The form is used by physicians and allied health professionals to.
Form Version 02/12 Will Replace The Current Cms 1500 Claim Form, 08/05, Effective With Claims.
To view instructions, hover over each field. Web how to submit claims: Fill out the health insurance claim form online and print it out for free. Web cms 1500 (02/12) claim form instructions cms 1500 (02/12) claim form instructions note:
Ad Access Any Form You Need.
State the type of health insurance applicable to. Web cms 1500 claim form instructions tool. This form is the only version. Complete, edit or print your forms instantly.
Claims May Be Electronically Submitted To A Medicare Carrier, Durable Medical Equipment Medicare Administrative Contractor (Dmemac), Or.
Web revised cms 1500 claim form, version 02/12. For complete instructions, refer to chapter 6 of the dme supplier manual. In order to increase health care provider participation in the workers' compensation system and improve injured workers' access to timely, quality medical. Insured’s name (last name, first name, middle initial).