Covid Consent Form
Covid Consent Form - *ages 12 years and older *question #12 pertain to bivalent booster dose eligibility for those who have completed a primary series of pfizer, moderna, novavax or janssen or those who have received a previous monovalent booster. Web by my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by law or state/federal guidance, employed or contracted by albertsons companies or one of its affiliated pharmacies and to be contacted at the number provided Find a vaccine near you. 5 june 2023 date last updated: If you're having problems using a document with your accessibility tools, please contact us for help. Since applicable medical consent laws are a matter of state, tribal, or territorial law, providers are advised to consult with their legal counsel to assure compliance with the scope of those consent laws. Take precautions regardless of your vaccination status. These steps help prevent spreading the virus to others in your household and your community. (clinic, health department, pharmacy, etc.,)_____ address:_____city:_____county:_____ state:_____ zip code: Below you will find the moderna vaccine screening and consent forms:
5 june 2023 date last updated: Text your zip code to 438829. Below you will find the moderna vaccine screening and consent forms: If you're having problems using a document with your accessibility tools, please contact us for help. Take precautions regardless of your vaccination status. Find a vaccine near you. Web by my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by law or state/federal guidance, employed or contracted by albertsons companies or one of its affiliated pharmacies and to be contacted at the number provided *ages 12 years and older *question #12 pertain to bivalent booster dose eligibility for those who have completed a primary series of pfizer, moderna, novavax or janssen or those who have received a previous monovalent booster. (clinic, health department, pharmacy, etc.,)_____ address:_____city:_____county:_____ state:_____ zip code: Message & data rates may apply.
Web by my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by law or state/federal guidance, employed or contracted by albertsons companies or one of its affiliated pharmacies and to be contacted at the number provided These steps help prevent spreading the virus to others in your household and your community. Text your zip code to 438829. *ages 12 years and older *question #12 pertain to bivalent booster dose eligibility for those who have completed a primary series of pfizer, moderna, novavax or janssen or those who have received a previous monovalent booster. 5 june 2023 date last updated: Message & data rates may apply. Find a vaccine near you. Below you will find the moderna vaccine screening and consent forms: Since applicable medical consent laws are a matter of state, tribal, or territorial law, providers are advised to consult with their legal counsel to assure compliance with the scope of those consent laws. If you're having problems using a document with your accessibility tools, please contact us for help.

COVID19 Vaccine Information Blackbutt Doctors Surgery
Web by my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by law or state/federal guidance, employed or contracted by albertsons companies or one of its affiliated pharmacies and to be contacted at the number provided If you're having problems using a.
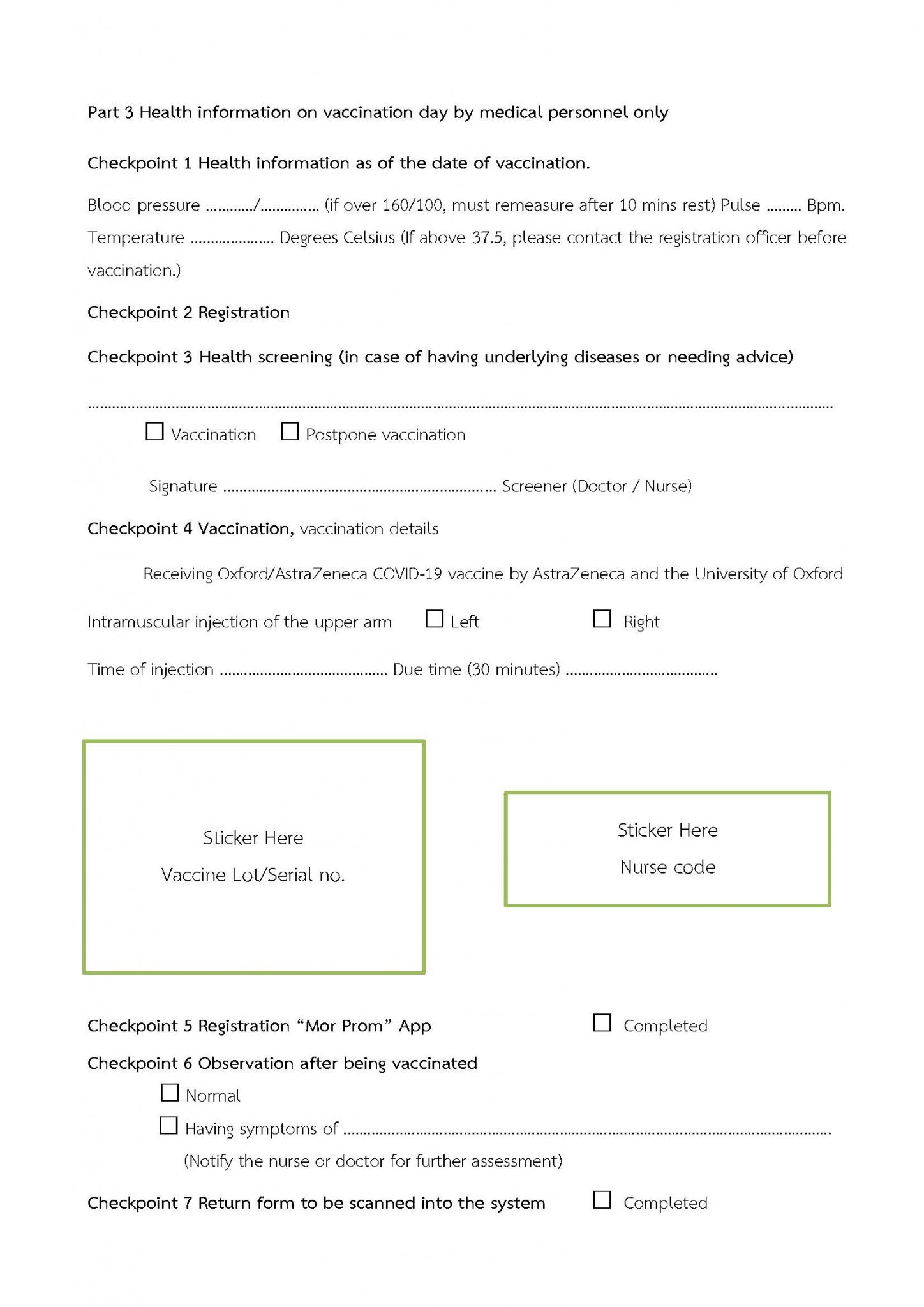
Consent Form and Vaccination Records Form for Coronavirus 2019 (COVID
*ages 12 years and older *question #12 pertain to bivalent booster dose eligibility for those who have completed a primary series of pfizer, moderna, novavax or janssen or those who have received a previous monovalent booster. Web by my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or.
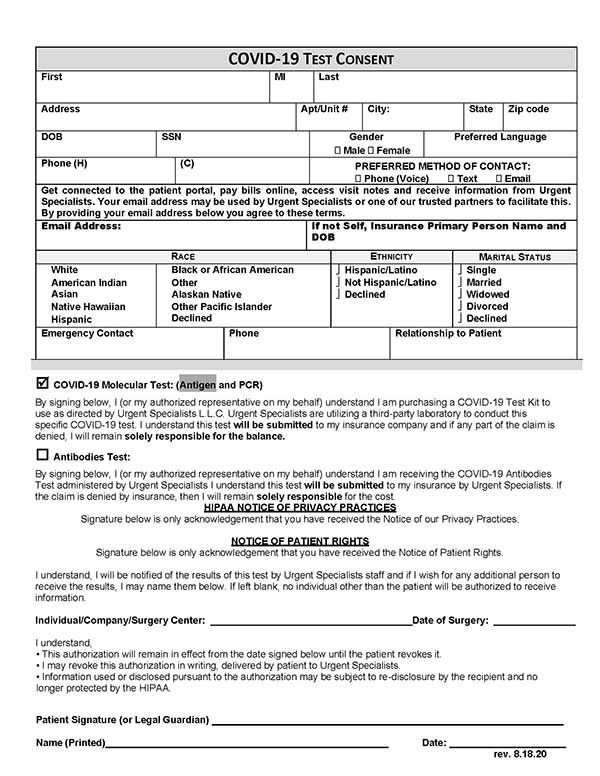
Urgent Specialists Occupational Health Services Forms
Find a vaccine near you. Web by my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by law or state/federal guidance, employed or contracted by albertsons companies or one of its affiliated pharmacies and to be contacted at the number provided These.

Minor Covid testing consent form St. Anthony's High School
Since applicable medical consent laws are a matter of state, tribal, or territorial law, providers are advised to consult with their legal counsel to assure compliance with the scope of those consent laws. *ages 12 years and older *question #12 pertain to bivalent booster dose eligibility for those who have completed a primary series of pfizer, moderna, novavax or janssen.
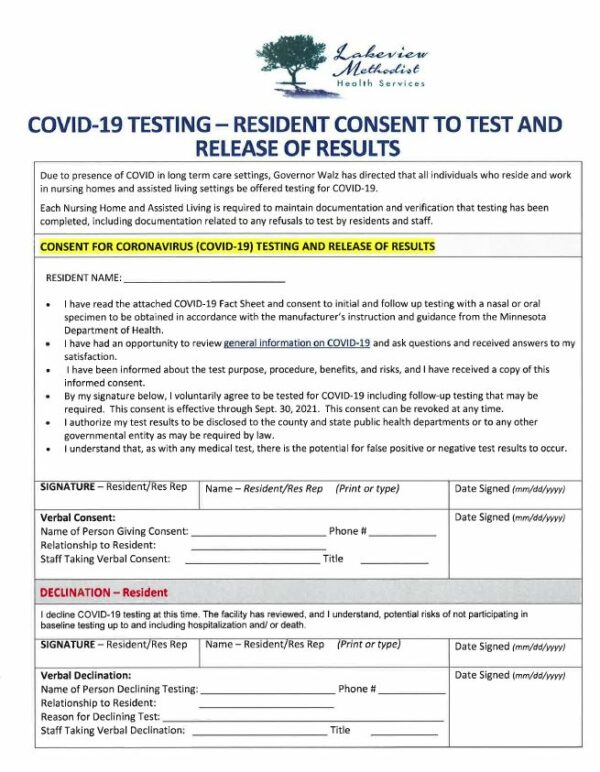
Covid19 Testing Resident Consent to Test and Release of Results
If you're having problems using a document with your accessibility tools, please contact us for help. Find a vaccine near you. Since applicable medical consent laws are a matter of state, tribal, or territorial law, providers are advised to consult with their legal counsel to assure compliance with the scope of those consent laws. Message & data rates may apply..
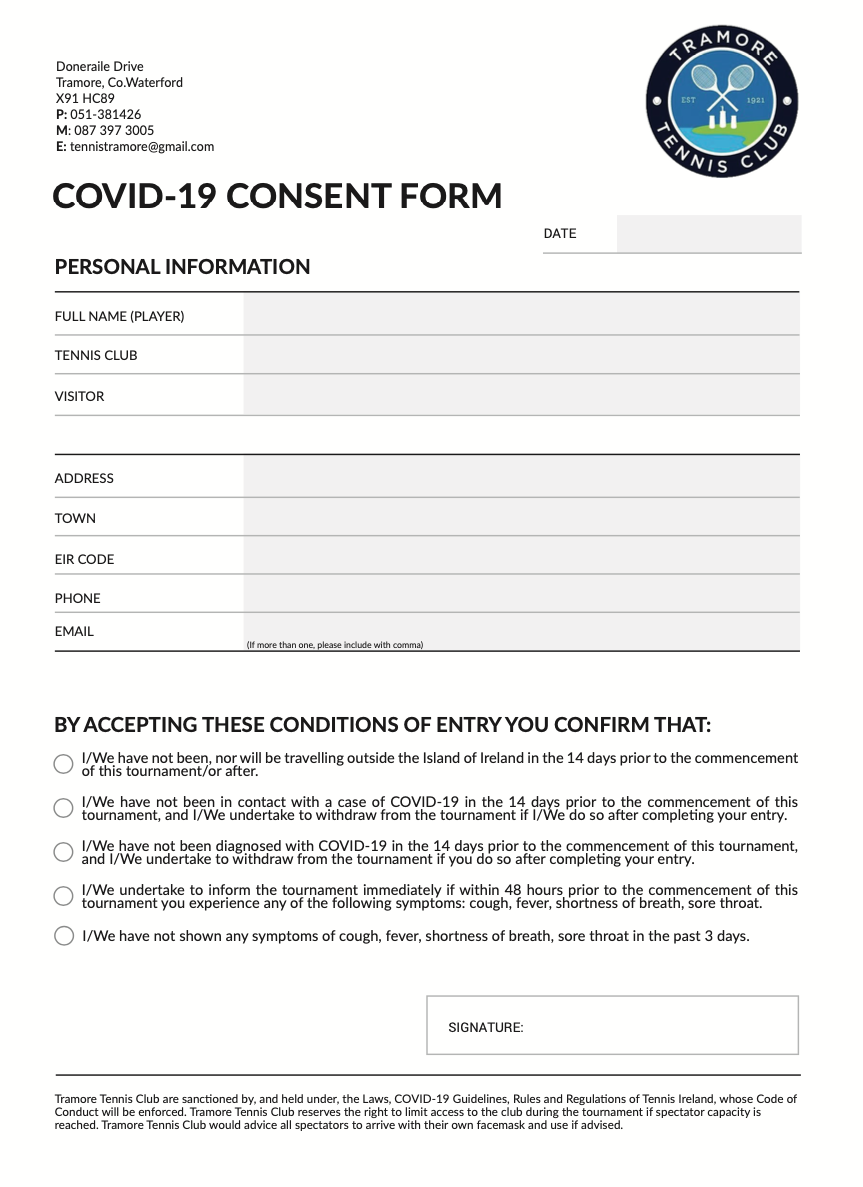
COVID19 Consent Form Tramore Tennis Club
Since applicable medical consent laws are a matter of state, tribal, or territorial law, providers are advised to consult with their legal counsel to assure compliance with the scope of those consent laws. *ages 12 years and older *question #12 pertain to bivalent booster dose eligibility for those who have completed a primary series of pfizer, moderna, novavax or janssen.

FWCS to offer COVID19 vaccines to students 16 and older WANE 15
Web by my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by law or state/federal guidance, employed or contracted by albertsons companies or one of its affiliated pharmacies and to be contacted at the number provided These steps help prevent spreading the.

Patient Forms
Message & data rates may apply. Web by my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by law or state/federal guidance, employed or contracted by albertsons companies or one of its affiliated pharmacies and to be contacted at the number provided.
consent form Riverside Remedies
5 june 2023 date last updated: (clinic, health department, pharmacy, etc.,)_____ address:_____city:_____county:_____ state:_____ zip code: Below you will find the moderna vaccine screening and consent forms: Web by my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by law or state/federal guidance,.

COVID19 Updates allengray
Find a vaccine near you. Message & data rates may apply. Text your zip code to 438829. Below you will find the moderna vaccine screening and consent forms: If you're having problems using a document with your accessibility tools, please contact us for help.
Below You Will Find The Moderna Vaccine Screening And Consent Forms:
5 june 2023 date last updated: If you're having problems using a document with your accessibility tools, please contact us for help. These steps help prevent spreading the virus to others in your household and your community. (clinic, health department, pharmacy, etc.,)_____ address:_____city:_____county:_____ state:_____ zip code:
*Ages 12 Years And Older *Question #12 Pertain To Bivalent Booster Dose Eligibility For Those Who Have Completed A Primary Series Of Pfizer, Moderna, Novavax Or Janssen Or Those Who Have Received A Previous Monovalent Booster.
Message & data rates may apply. Take precautions regardless of your vaccination status. Find a vaccine near you. Since applicable medical consent laws are a matter of state, tribal, or territorial law, providers are advised to consult with their legal counsel to assure compliance with the scope of those consent laws.
Web By My Signature Below, I Consent To The Administration Of The Vaccine(S) By A Pharmacist Or A Supervised Student Pharmacist Or Technician, Or Other Authorized Person, Where Permitted By Law Or State/Federal Guidance, Employed Or Contracted By Albertsons Companies Or One Of Its Affiliated Pharmacies And To Be Contacted At The Number Provided
Text your zip code to 438829.