Diabetic Shoe Order Form
Diabetic Shoe Order Form - Toe filler l5000 order form. The ordering provider can be your doctor, podiatrist, nurse practitioner, physician assistant or clinical nurse specialist. Web coverage of therapeutic shoes for persons with diabetes is based on social security act §1862(a)(1)(a) provisions (i.e. This template is designed to assist a physician (md or do) in completing a statement of certifying physician for therapeutic shoes, modifications, and inserts for persons with diabetes to meet requirements for medicare eligibility and coverage. Primary/managing physician packet for shoes and inserts. Web diabetic insert order form. Web check out our resource center to find additional documentation and forms that you’ll need for participation and reimbursement in the diabetic shoe program. Abn for shoes & inserts. Web you can use the printable clinical templates and suggested clinical data elements (cdes) for the. Web podiatric packet for shoes & inserts.
“reasonable and necessary”) and coverage of therapeutic shoes and inserts under the therapeutic shoes for individuals with diabetes benefit (social security act §1861(s)(12)). Primary/managing physician packet for shoes and inserts. Toe filler l5000 order form. Web podiatric packet for shoes & inserts. • open/download word docx file. The ordering provider can be your doctor, podiatrist, nurse practitioner, physician assistant or clinical nurse specialist. This template is designed to assist a physician (md or do) in completing a statement of certifying physician for therapeutic shoes, modifications, and inserts for persons with diabetes to meet requirements for medicare eligibility and coverage. • open/download word docx file. A statement of certifying physician completed by the md/do treating your diabetic condition, signed within the last 3 months. Abn for shoes & inserts.
Web you can use the printable clinical templates and suggested clinical data elements (cdes) for the. A5512 heat moldable insole order form. This template is designed to assist a physician (md or do) in completing a statement of certifying physician for therapeutic shoes, modifications, and inserts for persons with diabetes to meet requirements for medicare eligibility and coverage. Web coverage of therapeutic shoes for persons with diabetes is based on social security act §1862(a)(1)(a) provisions (i.e. Web diabetic insert order form. Total contact orthoses order form. Web a standard written order (page 3) this document specifies the item(s) that the ordering provider is requesting be provided to you. • open/download word docx file. Web check out our resource center to find additional documentation and forms that you’ll need for participation and reimbursement in the diabetic shoe program. Toe filler l5000 order form.

22+ Diabetic Shoes Covered By Medicare
• open/download word docx file. Web diabetic insert order form. A statement of certifying physician completed by the md/do treating your diabetic condition, signed within the last 3 months. Web a standard written order (page 3) this document specifies the item(s) that the ordering provider is requesting be provided to you. “reasonable and necessary”) and coverage of therapeutic shoes and.
Diabetic Footwear If The Shoe Fits, Wear It WCEI Blog WCEI Blog
Web diabetic insert order form. Web coverage of therapeutic shoes for persons with diabetes is based on social security act §1862(a)(1)(a) provisions (i.e. A statement of certifying physician completed by the md/do treating your diabetic condition, signed within the last 3 months. Web a standard written order (page 3) this document specifies the item(s) that the ordering provider is requesting.

Pin on Shoes dad
The ordering provider can be your doctor, podiatrist, nurse practitioner, physician assistant or clinical nurse specialist. Web check out our resource center to find additional documentation and forms that you’ll need for participation and reimbursement in the diabetic shoe program. • open/download word docx file. Web a standard written order (page 3) this document specifies the item(s) that the ordering.
Shoe Order Form Fillable Text Only Pdf Letter Size Instant Etsy
A statement of certifying physician completed by the md/do treating your diabetic condition, signed within the last 3 months. Web a standard written order (page 3) this document specifies the item(s) that the ordering provider is requesting be provided to you. • open/download word docx file. This template is designed to assist a physician (md or do) in completing a.

PS Diabetic Shoe Prescription Form by Alan DeFever Issuu
Web podiatric packet for shoes & inserts. • open/download word docx file. Toe filler l5000 order form. Web coverage of therapeutic shoes for persons with diabetes is based on social security act §1862(a)(1)(a) provisions (i.e. • open/download word docx file.

Pin on Diabetic Foot
A statement of certifying physician completed by the md/do treating your diabetic condition, signed within the last 3 months. Web you can use the printable clinical templates and suggested clinical data elements (cdes) for the. “reasonable and necessary”) and coverage of therapeutic shoes and inserts under the therapeutic shoes for individuals with diabetes benefit (social security act §1861(s)(12)). The ordering.

Foot and Ankle Problems By Dr. Richard Blake Nice Article on Finding
Abn for shoes & inserts. Web diabetic insert order form. Primary/managing physician packet for shoes and inserts. Web you can use the printable clinical templates and suggested clinical data elements (cdes) for the. • open/download word docx file.
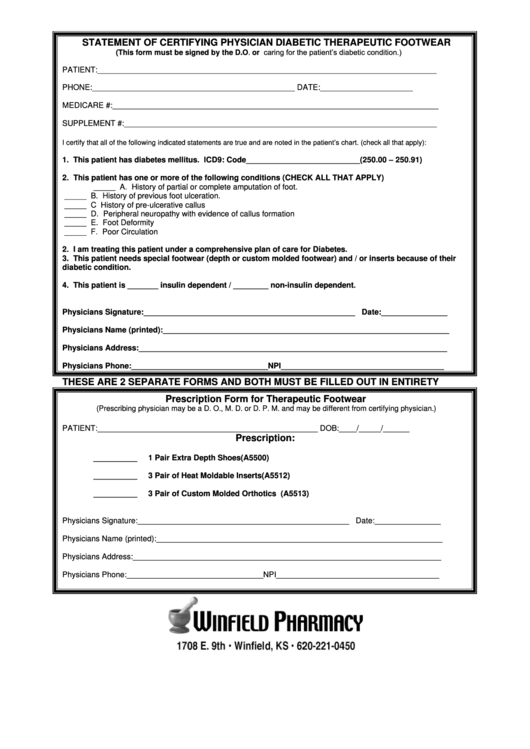
Statement Of Certifying Physician Diabetic Therapeutic Footwear
• open/download word docx file. Web a standard written order (page 3) this document specifies the item(s) that the ordering provider is requesting be provided to you. Toe filler l5000 order form. Abn for shoes & inserts. Web you can use the printable clinical templates and suggested clinical data elements (cdes) for the.
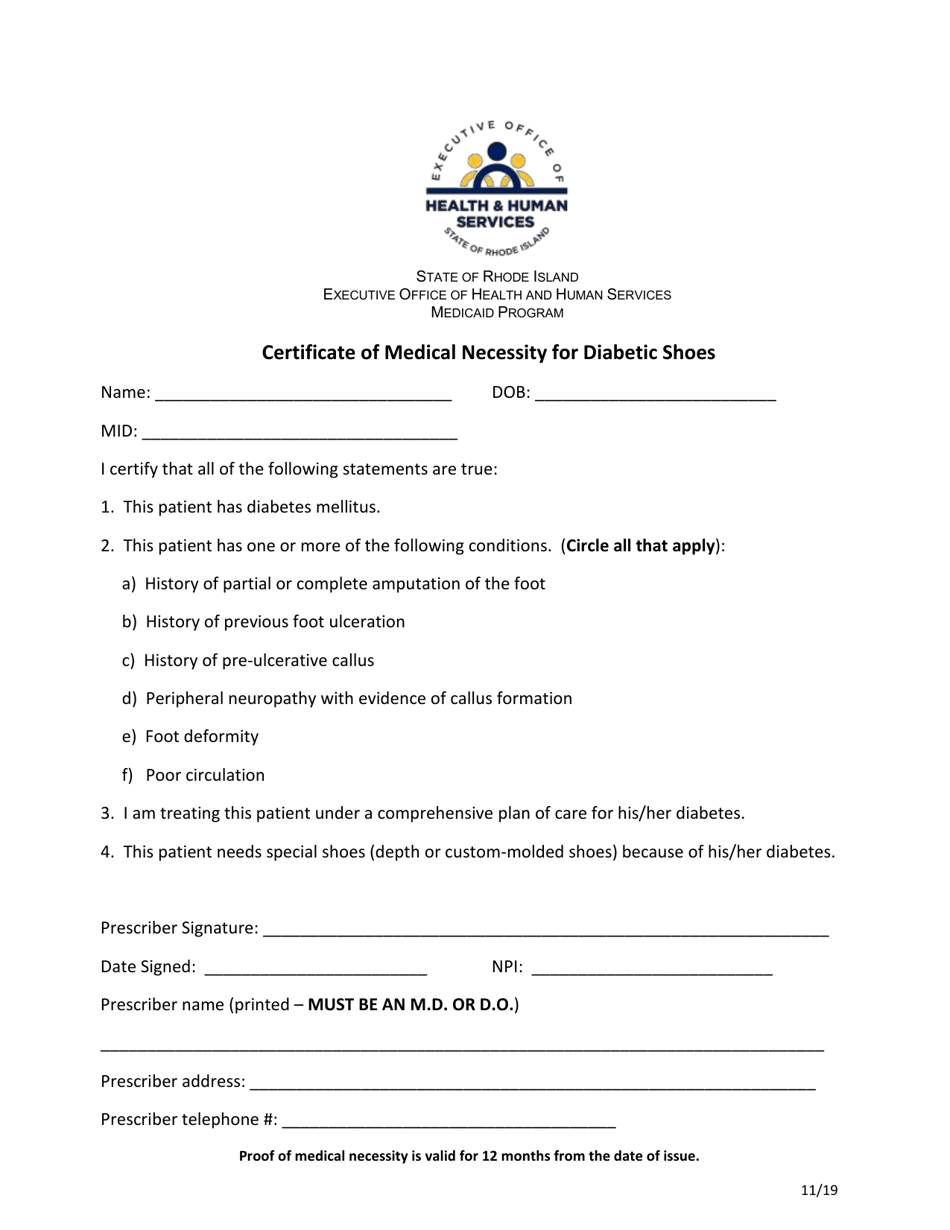
Rhode Island Certificate of Medical Necessity for Diabetic Shoes
The ordering provider can be your doctor, podiatrist, nurse practitioner, physician assistant or clinical nurse specialist. Web podiatric packet for shoes & inserts. Web coverage of therapeutic shoes for persons with diabetes is based on social security act §1862(a)(1)(a) provisions (i.e. • open/download word docx file. Total contact orthoses order form.

Online InStride Diabetic Shoe Order Doc Template pdfFiller
Total contact orthoses order form. This template is designed to assist a physician (md or do) in completing a statement of certifying physician for therapeutic shoes, modifications, and inserts for persons with diabetes to meet requirements for medicare eligibility and coverage. The ordering provider can be your doctor, podiatrist, nurse practitioner, physician assistant or clinical nurse specialist. • open/download word.
Web Podiatric Packet For Shoes & Inserts.
A5512 heat moldable insole order form. Toe filler l5000 order form. Primary/managing physician packet for shoes and inserts. This template is designed to assist a physician (md or do) in completing a statement of certifying physician for therapeutic shoes, modifications, and inserts for persons with diabetes to meet requirements for medicare eligibility and coverage.
“Reasonable And Necessary”) And Coverage Of Therapeutic Shoes And Inserts Under The Therapeutic Shoes For Individuals With Diabetes Benefit (Social Security Act §1861(S)(12)).
• open/download word docx file. • open/download word docx file. Web check out our resource center to find additional documentation and forms that you’ll need for participation and reimbursement in the diabetic shoe program. Web you can use the printable clinical templates and suggested clinical data elements (cdes) for the.
The Ordering Provider Can Be Your Doctor, Podiatrist, Nurse Practitioner, Physician Assistant Or Clinical Nurse Specialist.
Abn for shoes & inserts. Web diabetic insert order form. Web coverage of therapeutic shoes for persons with diabetes is based on social security act §1862(a)(1)(a) provisions (i.e. Web a standard written order (page 3) this document specifies the item(s) that the ordering provider is requesting be provided to you.
Total Contact Orthoses Order Form.
A statement of certifying physician completed by the md/do treating your diabetic condition, signed within the last 3 months.