Fl2 Nc Form
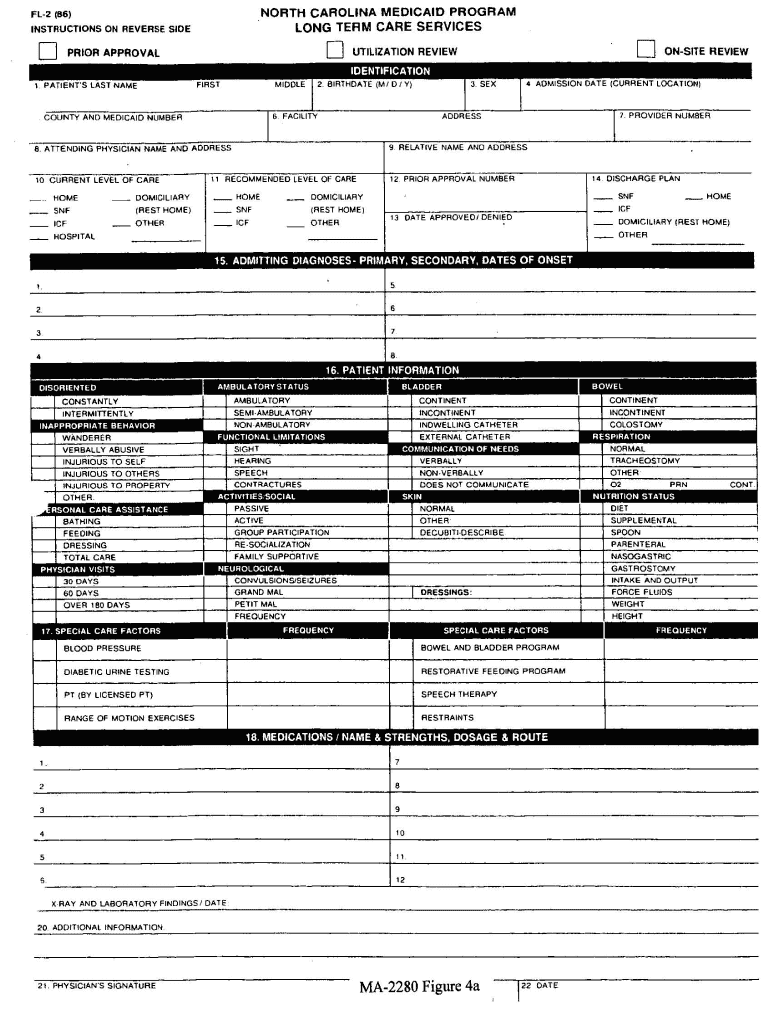
Fl2 Nc Form - Physician, hospital discharge planner, social worker, etc.) should advise the facility that he or she is initiating an fl2 requesting prior approval for nursing facility care. Web the referral source submits the north carolina level i screening form via ncmust. Providers must use one of the following forms to submit the md signature: County and medicaid number 6. Web north carolina level i screening form for nursing facility admissions. Web providers can upload the fl2 form with the electronic fl2 prior approval request or they can complete the electronic fl2 portal submission and upload the physician signature form. Admission date (current location) 5. The following forms are found on the nctracks provider prior approval webpage. Attending physician name and address 9. How do i submit an attachment or supplemental material for my pa?
Health benefits/nc medicaid (dhb) form effective date. Providers must use one of the following forms to submit the md signature: Web north carolina level i screening form for nursing facility admissions. Attending physician name and address 9. Web providers can upload the fl2 form with the electronic fl2 prior approval request or they can complete the electronic fl2 portal submission and upload the physician signature form. The following forms are found on the nctracks provider prior approval webpage. County and medicaid number 6. Web long term care (ltc) prior approval (pa) requests require a valid physician (md) signature that is dated within 30 calendar days prior to the date of submission. Web the referral source submits the north carolina level i screening form via ncmust. Web nc medicaid long term care fl2 form recipient information recipient last name:
County and medicaid number 6. The following forms are found on the nctracks provider prior approval webpage. Web north carolina level i screening form for nursing facility admissions. Providers must use one of the following forms to submit the md signature: Admission date (current location) 5. Web long term care (ltc) prior approval (pa) requests require a valid physician (md) signature that is dated within 30 calendar days prior to the date of submission. Attending physician name and address 9. Web nc medicaid long term care fl2 form recipient information recipient last name: Web providers can upload the fl2 form with the electronic fl2 prior approval request or they can complete the electronic fl2 portal submission and upload the physician signature form. Health benefits/nc medicaid (dhb) form effective date.

Fill Free fillable forms for the state of North Carolina
Providers must use one of the following forms to submit the md signature: County and medicaid number 6. Web the referral source submits the north carolina level i screening form via ncmust. Health benefits/nc medicaid (dhb) form effective date. Web long term care (ltc) prior approval (pa) requests require a valid physician (md) signature that is dated within 30 calendar.

Fill Free fillable forms for the state of North Carolina
Health benefits/nc medicaid (dhb) form effective date. Web nc medicaid long term care fl2 form recipient information recipient last name: Web long term care (ltc) prior approval (pa) requests require a valid physician (md) signature that is dated within 30 calendar days prior to the date of submission. Providers must use one of the following forms to submit the md.
Fl2 Form Fill Out and Sign Printable PDF Template signNow
County and medicaid number 6. Web providers can upload the fl2 form with the electronic fl2 prior approval request or they can complete the electronic fl2 portal submission and upload the physician signature form. Web the referral source submits the north carolina level i screening form via ncmust. How do i submit an attachment or supplemental material for my pa?.
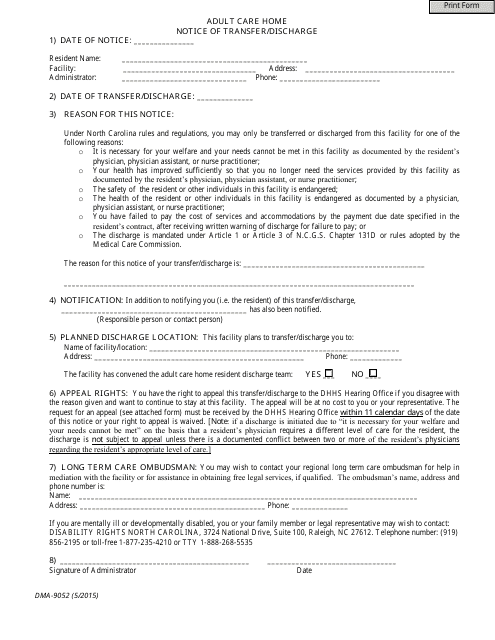
Form DMA9052 Download Fillable PDF, Adult Care Home Notice of Transfer
Attending physician name and address 9. Web nc medicaid long term care fl2 form recipient information recipient last name: Web providers can upload the fl2 form with the electronic fl2 prior approval request or they can complete the electronic fl2 portal submission and upload the physician signature form. County and medicaid number 6. Providers must use one of the following.

2012 Form NC DoR NC4 Fill Online, Printable, Fillable, Blank PDFfiller
The following forms are found on the nctracks provider prior approval webpage. Admission date (current location) 5. Health benefits/nc medicaid (dhb) form effective date. Web providers can upload the fl2 form with the electronic fl2 prior approval request or they can complete the electronic fl2 portal submission and upload the physician signature form. Web north carolina level i screening form.
Nc Fl2 Form ≡ Fill Out Printable PDF Forms Online
Web the referral source submits the north carolina level i screening form via ncmust. Web long term care (ltc) prior approval (pa) requests require a valid physician (md) signature that is dated within 30 calendar days prior to the date of submission. Attending physician name and address 9. Health benefits/nc medicaid (dhb) form effective date. Web nc medicaid long term.
Fuel Log FL2 Customizable Form Template Forms Direct
County and medicaid number 6. Providers must use one of the following forms to submit the md signature: Admission date (current location) 5. How do i submit an attachment or supplemental material for my pa? Web the referral source submits the north carolina level i screening form via ncmust.

Fl2 Form Nc Fill Online, Printable, Fillable, Blank pdfFiller
Web the referral source submits the north carolina level i screening form via ncmust. Attending physician name and address 9. The following forms are found on the nctracks provider prior approval webpage. Web north carolina level i screening form for nursing facility admissions. Providers must use one of the following forms to submit the md signature:

Fill Free fillable forms for the state of North Carolina
Web providers can upload the fl2 form with the electronic fl2 prior approval request or they can complete the electronic fl2 portal submission and upload the physician signature form. The following forms are found on the nctracks provider prior approval webpage. Web north carolina level i screening form for nursing facility admissions. Admission date (current location) 5. How do i.

Fill Free fillable forms for the state of North Carolina
County and medicaid number 6. Web long term care (ltc) prior approval (pa) requests require a valid physician (md) signature that is dated within 30 calendar days prior to the date of submission. Web providers can upload the fl2 form with the electronic fl2 prior approval request or they can complete the electronic fl2 portal submission and upload the physician.
Web Nc Medicaid Long Term Care Fl2 Form Recipient Information Recipient Last Name:
Web north carolina level i screening form for nursing facility admissions. Web long term care (ltc) prior approval (pa) requests require a valid physician (md) signature that is dated within 30 calendar days prior to the date of submission. Providers must use one of the following forms to submit the md signature: Web the referral source submits the north carolina level i screening form via ncmust.
Physician, Hospital Discharge Planner, Social Worker, Etc.) Should Advise The Facility That He Or She Is Initiating An Fl2 Requesting Prior Approval For Nursing Facility Care.
Admission date (current location) 5. Web providers can upload the fl2 form with the electronic fl2 prior approval request or they can complete the electronic fl2 portal submission and upload the physician signature form. The following forms are found on the nctracks provider prior approval webpage. How do i submit an attachment or supplemental material for my pa?
County And Medicaid Number 6.
Health benefits/nc medicaid (dhb) form effective date. Attending physician name and address 9.