Florida Blue Claim Form
Florida Blue Claim Form - You can submit your claim any time during the year. You can submit your claim any time during the year. Web 2 up to $500 in rewards towards your premium or other medical expenses. Web english authorized representative designation form use this form to select an individual or entity to act on your behalf during the disputed claims process. You can submit your claim any time during the year. Send completed form & pharmacy receipts to: Web mail completed claim form to: Vast network of doctors, providers, speialists and hospitals. Quality care network 3 access to our large network of doctors, specialists and care programs at no extra cost. English medicare reimbursement account (mra) pay me back claim form
Vast network of doctors, providers, speialists and hospitals. Find and download forms often used by our members. Quality care network 3 access to our large network of doctors, specialists and care programs at no extra cost. The completion and submission of this form does not guarantee eligibility for benefits. Attach explanation of benefits (if applicable) and prescription receipts. Web forms for members enrolled in individual, family and employer plans with florida blue. Web prescription drug claim form directions: Web 2 up to $500 in rewards towards your premium or other medical expenses. You must file your claim within one year from the date of service. You can submit your claim any time during the year.
Use a separate form for each patient. With florida blue it pays to stay healthy! You must file your claim within one year from the date of service. Complete and sign claim form below. (bcbsf) that certain services provided to bcbsf’s members by providers are not covered services because they are not medically necessary or experimental or investigational in nature. Medical, vision, dental claims and reimbursement forms prescription drug forms coverage and premium payment forms personal information forms medicare forms hipaa. The completion and submission of this form does not guarantee eligibility for benefits. Attach explanation of benefits (if applicable) and prescription receipts. You can submit your claim any time during the year. Web 2 up to $500 in rewards towards your premium or other medical expenses.
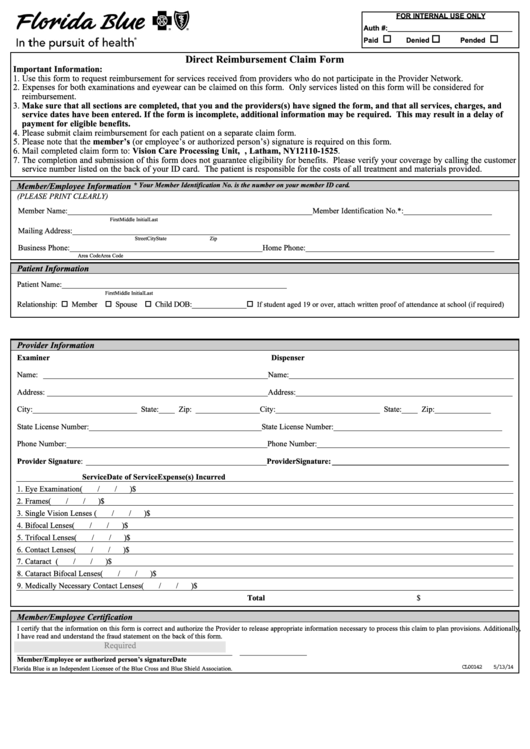
Direct Reimbursement Claim Form Florida Blue printable pdf download
English medicare reimbursement account (mra) pay me back claim form Quality care network 3 access to our large network of doctors, specialists and care programs at no extra cost. You can submit your claim any time during the year. You can submit your claim any time during the year. Complete and sign claim form below.
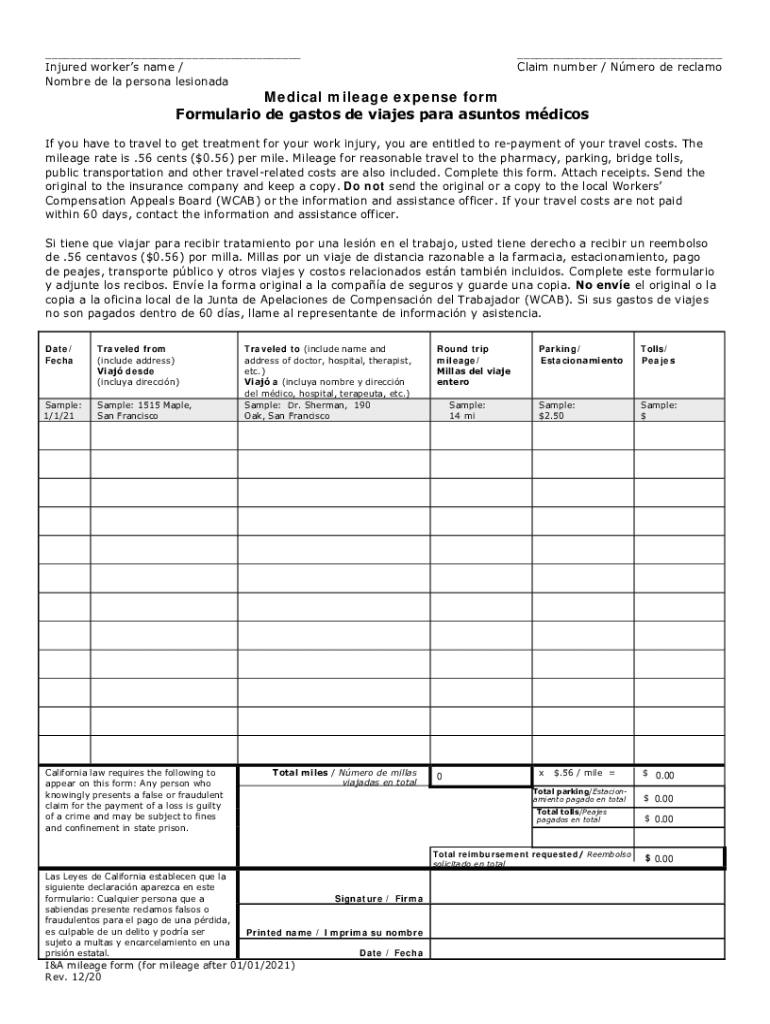
CA I&A Mileage Form 20202022 Fill and Sign Printable Template Online
You must file your claim within one year from the date of service. Web forms for members enrolled in individual, family and employer plans with florida blue. Quality care network 3 access to our large network of doctors, specialists and care programs at no extra cost. Complete and sign claim form below. You can submit your claim any time during.
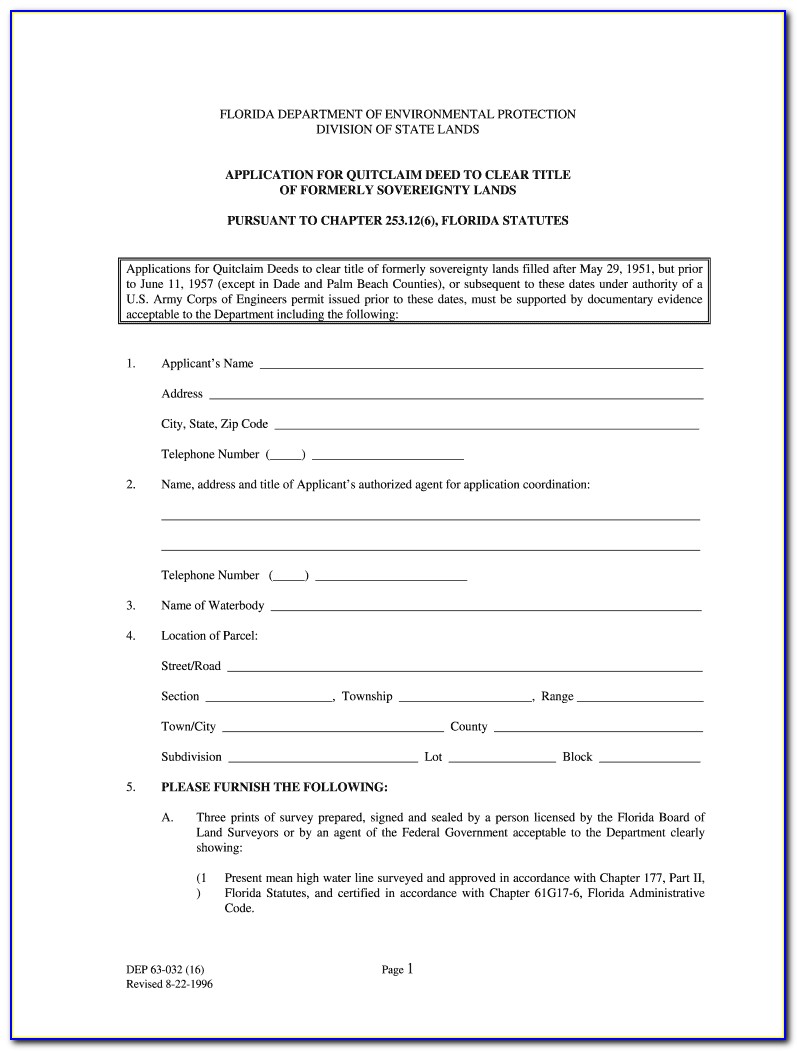
Florida Quit Claim Deed Form Free
English medicare reimbursement account (mra) pay me back claim form Vision care processing unit, p.o. You can submit your claim any time during the year. You can submit your claim any time during the year. You must file your claim within one year from the date of service.
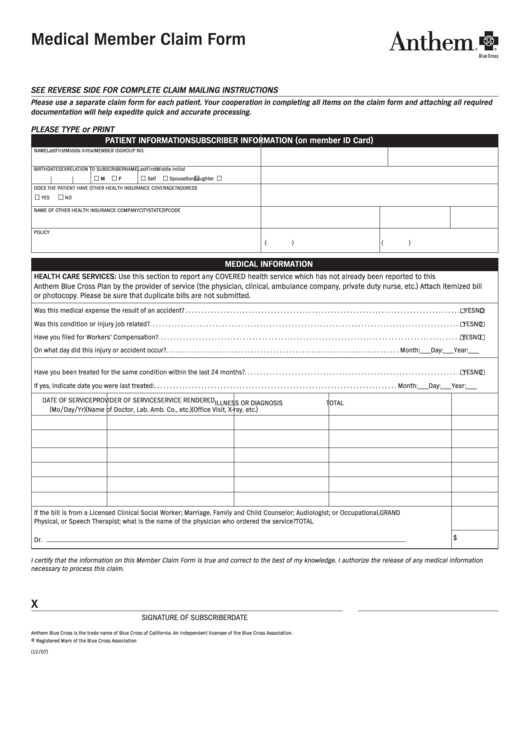
Medical Member Claim Form Blue Cross California printable pdf download
(bcbsf) that certain services provided to bcbsf’s members by providers are not covered services because they are not medically necessary or experimental or investigational in nature. You can submit your claim any time during the year. Complete and sign claim form below. Attach explanation of benefits (if applicable) and prescription receipts. You must file your claim within one year from.

Florida Statutory Quit Claim Deed Form Universal Network
Use a separate form for each patient. Attach explanation of benefits (if applicable) and prescription receipts. Quality care network 3 access to our large network of doctors, specialists and care programs at no extra cost. Web english authorized representative designation form use this form to select an individual or entity to act on your behalf during the disputed claims process..
Quit Claim Deed Florida Form Volusia County
You must file your claim within one year from the date of service. With florida blue it pays to stay healthy! Use a separate form for each patient. Web forms for members enrolled in individual, family and employer plans with florida blue. Please verify your coverage by calling the customer service number listed on the back of your id card.

Member Forms A&B Insurance and Financial
Web english authorized representative designation form use this form to select an individual or entity to act on your behalf during the disputed claims process. Expert agents across the state 4 Vast network of doctors, providers, speialists and hospitals. You must file your claim within one year from the date of service. Web 2 up to $500 in rewards towards.

Blue Cross Blue Shield Overseas Claim Form Fill Online, Printable
Web forms for members enrolled in individual, family and employer plans with florida blue. You can find detailed instructions on how to file an appeal in the disputed claims process document. Web mail completed claim form to: With florida blue it pays to stay healthy! You can submit your claim any time during the year.
Free Blue Cross Blue Shield Association Member Claim Form PDF 90KB
Web 2 up to $500 in rewards towards your premium or other medical expenses. Web english authorized representative designation form use this form to select an individual or entity to act on your behalf during the disputed claims process. Find and download forms often used by our members. English medicare reimbursement account (mra) pay me back claim form You can.
Quit Claim Deed Florida Form Free Form Resume Examples 4x2vyrjV5l
Find and download forms often used by our members. You can submit your claim any time during the year. Attach explanation of benefits (if applicable) and prescription receipts. Vision care processing unit, p.o. You can find detailed instructions on how to file an appeal in the disputed claims process document.
Expert Agents Across The State 4
You can submit your claim any time during the year. Quality care network 3 access to our large network of doctors, specialists and care programs at no extra cost. Send completed form & pharmacy receipts to: Web 2 up to $500 in rewards towards your premium or other medical expenses.
Web English Authorized Representative Designation Form Use This Form To Select An Individual Or Entity To Act On Your Behalf During The Disputed Claims Process.
Vast network of doctors, providers, speialists and hospitals. Web prescription drug claim form directions: With florida blue it pays to stay healthy! Please verify your coverage by calling the customer service number listed on the back of your id card.
(Bcbsf) That Certain Services Provided To Bcbsf’s Members By Providers Are Not Covered Services Because They Are Not Medically Necessary Or Experimental Or Investigational In Nature.
You must file your claim within one year from the date of service. Find and download forms often used by our members. Use a separate form for each patient. You can find detailed instructions on how to file an appeal in the disputed claims process document.
English Medicare Reimbursement Account (Mra) Pay Me Back Claim Form
The completion and submission of this form does not guarantee eligibility for benefits. You must file your claim within one year from the date of service. Vision care processing unit, p.o. You can submit your claim any time during the year.