Health First Prior Authorization Form
Health First Prior Authorization Form - Change of provider (cop) form; 2.please complete and fax this request form along with all supporting clinical. Find affordable health coverage here. If you have any questions, you can reach. Web authorization to release protected health information (phi) complete this form if you want to give someone (such as a family member, caregiver, or another. This form may be completed. Get your online template and fill it in using progressive features. 2021.how to complete change of provider form; Enjoy smart fillable fields and interactivity. Subscriber contracts & schedule of benefits (sob) healthfirst.
Web up to $40 cash back related to plan treatment authorization form care 1st arizona prior authorization form treatment authorization request ph 602.778.1800 (options 5, 6) fax. Covermymeds is healthfirst prior authorization forms’s preferred method for receiving epa requests. Web access the resources you need as an individual, family, or medicare advantage member. Enjoy smart fillable fields and interactivity. 2.please complete and fax this request form along with all supporting clinical. / patient information last name: Web authorization to release protected health information (phi) complete this form if you want to give someone (such as a family member, caregiver, or another. Web this is an update to the article titled ” signature updates to home health prior authorization request forms ,which was published on the texas medicaid &. Web 2022 provider resources. Prior authorization request (par) form inpatient par form:
Subscriber contracts & schedule of benefits (sob) healthfirst. To submit requests, please fax completed form to the utilization review department: 2021.how to complete change of provider form; Web provider prior authorization form fax medical authorization requests to: Web what is prior authorization? **please note that for plans with $0 cost share, all preferred. Covermymeds is healthfirst prior authorization forms’s preferred method for receiving epa requests. Web prior authorization request form. Enjoy smart fillable fields and interactivity. Web this is an update to the article titled ” signature updates to home health prior authorization request forms ,which was published on the texas medicaid &.
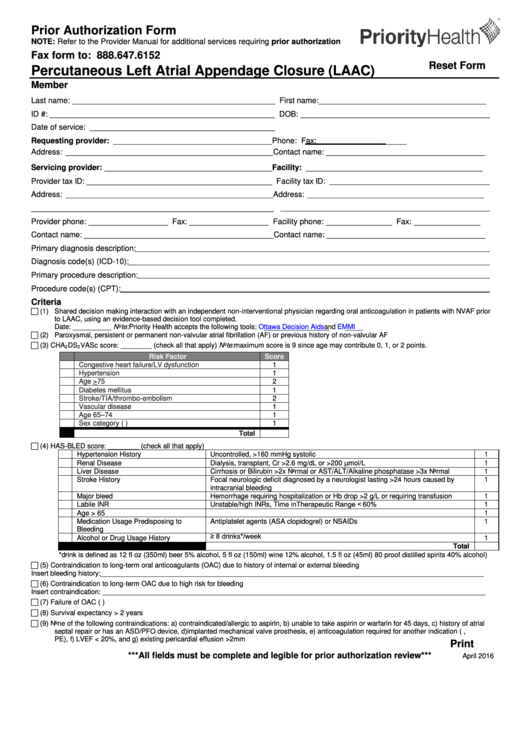
Top 5 Priority Health Prior Authorization Form Templates free to
An authorized agent is an employee of the prescribing. Web prior authorization in health care is a requirement that a healthcare provider (such as your primary care physician or a hospital) gets approval from your insurance. Web fax medical authorization requests to: Cvs caremark part d services. / patient information last name:
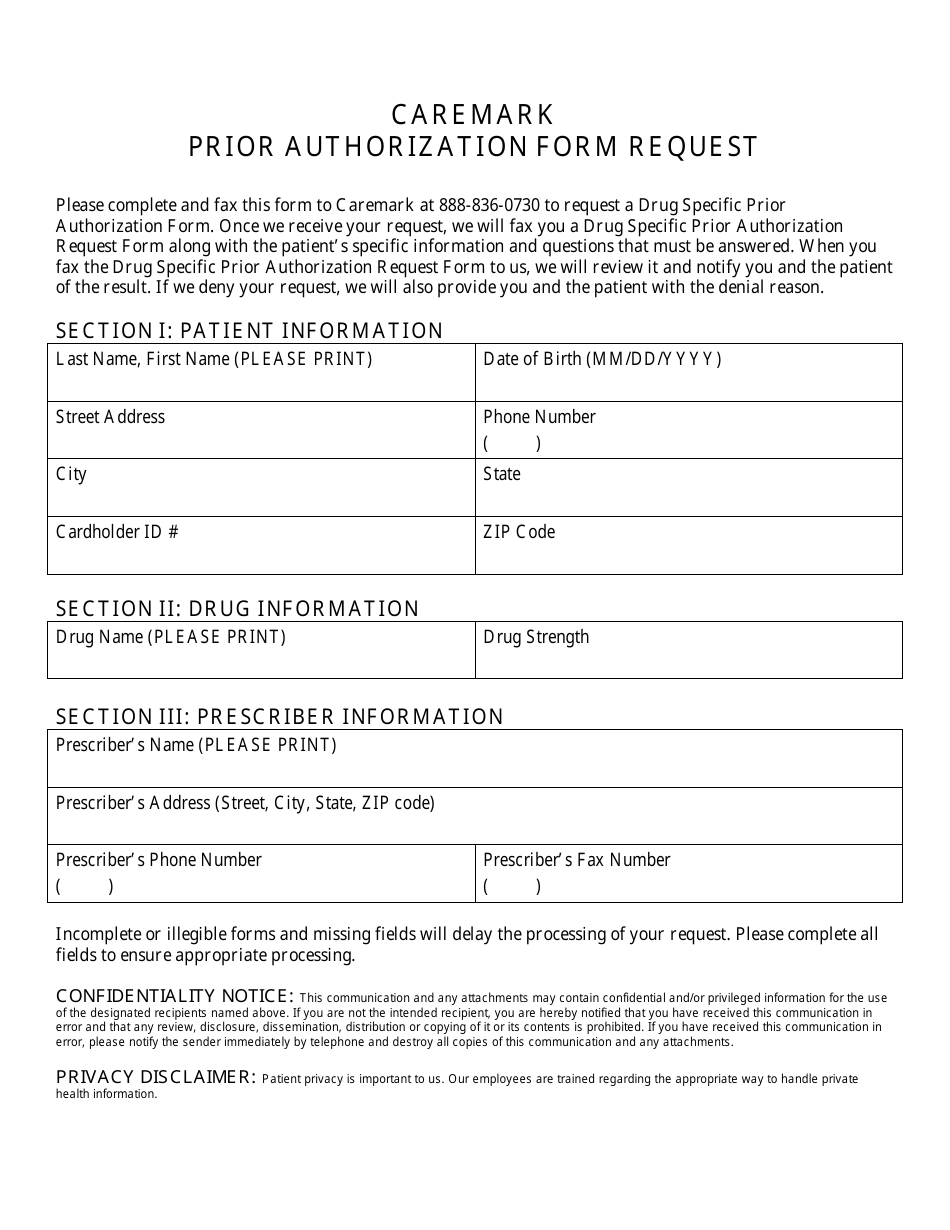
Prior Authorization Form Request Cvs Caremark Download Printable PDF
Prior authorization request (par) form inpatient par form: Web access the resources you need as an individual, family, or medicare advantage member. 2.please complete and fax this request form along with all supporting clinical. Web authorization to release protected health information (phi) complete this form if you want to give someone (such as a family member, caregiver, or another. For.
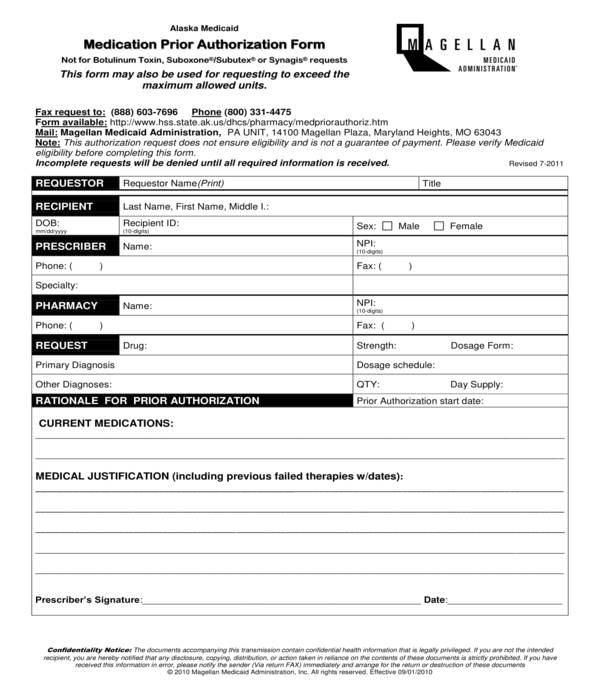
FREE 11+ Prior Authorization Forms in PDF MS Word
Web use this form when requesting prior authorization of therapy services for healthfirst members. / patient information last name: Covermymeds is healthfirst prior authorization forms’s preferred method for receiving epa requests. Web prior authorization request form. Find affordable health coverage here.
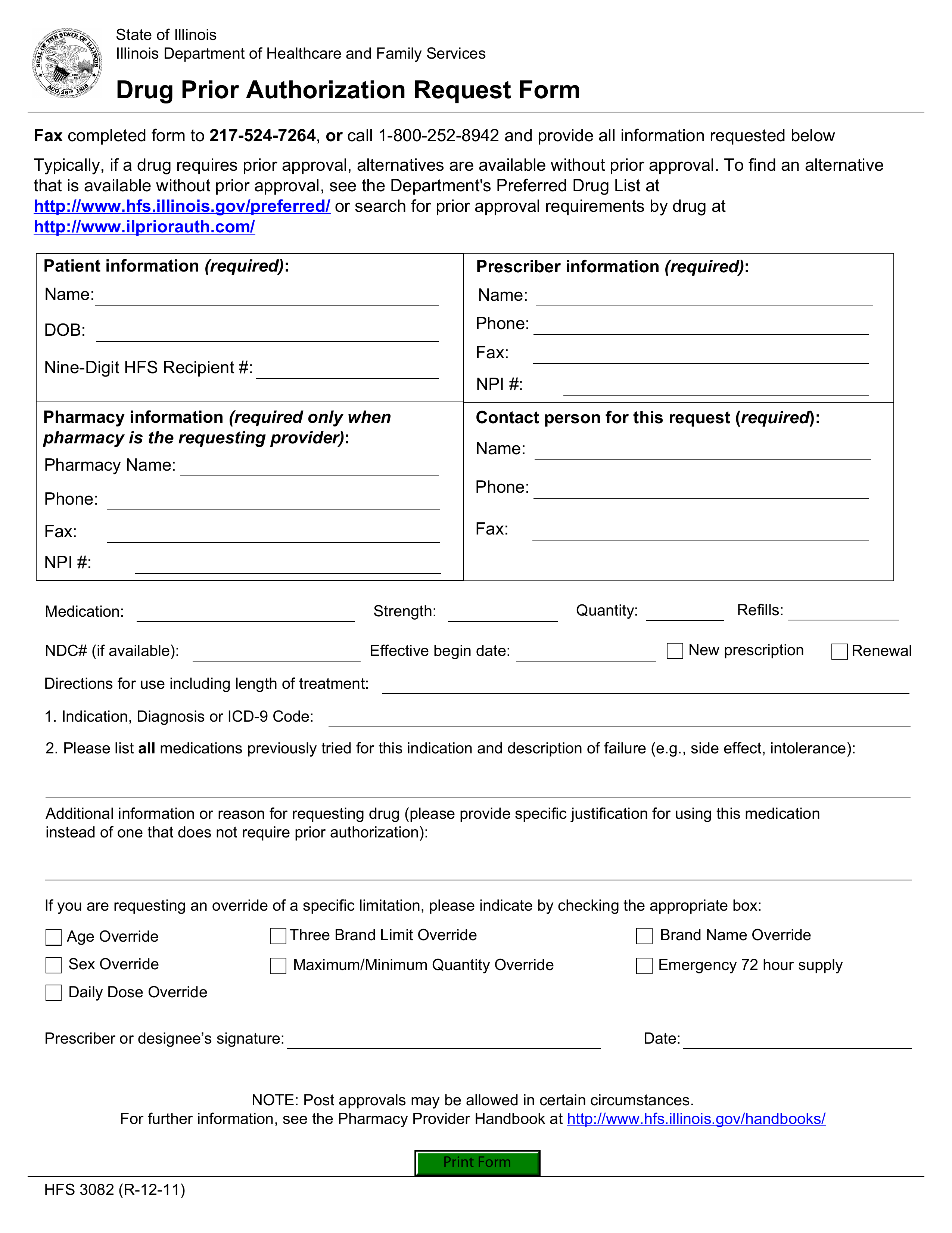
Free Illinois Medicaid Prior (Rx) Authorization Form PDF eForms
Web medical prior authorization list changes (small and large group commercial plans) updated july 1, 2022; Covermymeds is healthfirst prior authorization forms’s preferred method for receiving epa requests. Web fax medical authorization requests to: This form may be completed. Cvs caremark part d services.
Keystone First Universal Pharmacy Oral Prior Authorization Form 2020
Subscriber contracts & schedule of benefits (sob) healthfirst. Web up to $40 cash back related to plan treatment authorization form care 1st arizona prior authorization form treatment authorization request ph 602.778.1800 (options 5, 6) fax. Web select the appropriate healthfirst form to get started. Web provider prior authorization form fax medical authorization requests to: Web prior approval rate changes;
Medicare Authorization Form Download Fillable PDF Templateroller
2021.how to complete change of provider form; Web up to $40 cash back related to plan treatment authorization form care 1st arizona prior authorization form treatment authorization request ph 602.778.1800 (options 5, 6) fax. This form may be completed. Web use this form when requesting prior authorization of therapy services for healthfirst members. For some prescription medications, your doctor may.

FREE 41+ Authorization Forms in PDF Excel MS word
Change of provider (cop) form; Web provider prior authorization form fax medical authorization requests to: For some prescription medications, your doctor may need to get prior authorization from us before it’s approved for you to pick up at your pharmacy. Enjoy smart fillable fields and interactivity. To submit requests, please fax completed form to the utilization review department:
FREE 8+ Sample Prior Authorization Forms in PDF MS Word
Web prior authorization request and notification form honolulu, hi 96813.4100 t 808.532.4006 800.458.4600 f 866.572.4384 uhahealth.com prior authorization. Web select the appropriate healthfirst form to get started. Web this is an update to the article titled ” signature updates to home health prior authorization request forms ,which was published on the texas medicaid &. Web authorization to release protected health.
Top Florida Medicaid Prior Authorization Form Templates free to
For some prescription medications, your doctor may need to get prior authorization from us before it’s approved for you to pick up at your pharmacy. Enjoy smart fillable fields and interactivity. Web request for medicare prescription drug coverage determination. Web prior authorization request and notification form honolulu, hi 96813.4100 t 808.532.4006 800.458.4600 f 866.572.4384 uhahealth.com prior authorization. This form may.
Prior Authorization Request Form Fill Online, Printable, Fillable
Change of provider (cop) form; Web this is an update to the article titled ” signature updates to home health prior authorization request forms ,which was published on the texas medicaid &. Web prior authorization request form. Find affordable health coverage here. Web request for medicare prescription drug coverage determination.
Subscriber Contracts & Schedule Of Benefits (Sob) Healthfirst.
An authorized agent is an employee of the prescribing. Web this is an update to the article titled ” signature updates to home health prior authorization request forms ,which was published on the texas medicaid &. Web prior approval rate changes; Cvs caremark part d services.
Web Request For Medicare Prescription Drug Coverage Determination.
Web prior authorization request form. Enjoy smart fillable fields and interactivity. **please note that for plans with $0 cost share, all preferred. Web provider prior authorization form fax medical authorization requests to:
This Form May Be Completed.
For some prescription medications, your doctor may need to get prior authorization from us before it’s approved for you to pick up at your pharmacy. Find affordable health coverage here. Web what is prior authorization? 2021.how to complete change of provider form;
Web 2022 Provider Resources.
Web this form must be signed by the prescriber but can also be completed by the prescriber or his/her authorized agent. Web authorization to release protected health information (phi) complete this form if you want to give someone (such as a family member, caregiver, or another. Web use this form when requesting prior authorization of therapy services for healthfirst members. If you have any questions, you can reach.