Magellan Prior Authorization Form Pdf
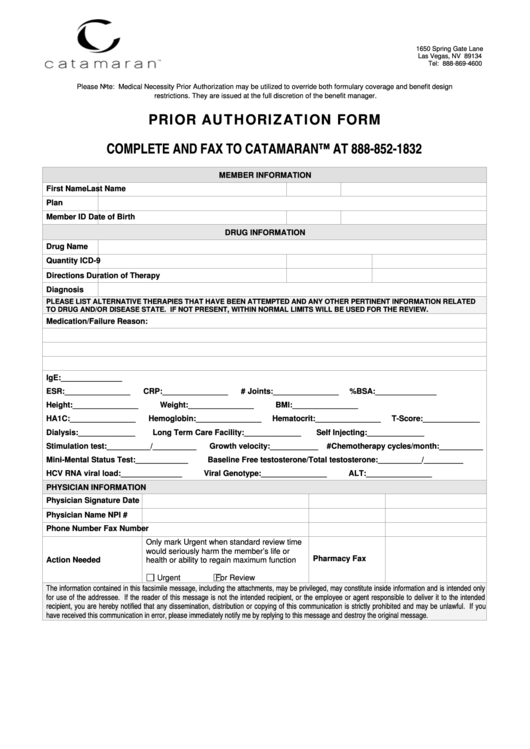
Magellan Prior Authorization Form Pdf - Request or access prior authorizations and view clinical guidelines. Web if you are not the patient or the prescriber, you will need to submit a phi disclosure authorization form with this request which can be found at the following link: Web when a service authorization is required, follow the magellan of virginia’s service authorization process by completing the applicable authorization request methodology [i.e., request higher level of care, service request application (sra), or treatment request form]. Select the appropriate magellan rx management form to get started. Web prior authorization request general pa form submit requests to: Instructions for retrospective review form; 0.1 mg/kg subcutaneous (sc) qd or qod up to 6 mg per day 1. Auxiliary forms (use as needed) Web prescription drug prior authorization form fax this form to: Treatment authorization request form for 90837 mental health and substance use disorder.
Web prescription drug prior authorization. You simply file your claim and respond to any outreach calls from a magellan, should such occur. Instructions for retrospective review form; Treatment authorization request form for 90837 mental health and substance use disorder. Required medical information drug/product name: Yes is this request for a yes continuation of therapy? Web magellan rx management prior authorization request form fax completed form to: Request or access prior authorizations and view clinical guidelines. 0.1 mg/kg subcutaneous (sc) qd or qod up to 6 mg per day 1. Web prescription drug prior authorization (pa) request form fax to magellan pharmacy solutions:
Web prescription drug prior authorization form fax this form to: Select the appropriate magellan rx management form to get started. Treatment authorization request form for 90837 mental health and substance use disorder. Request or access prior authorizations and view clinical guidelines. Web prescription drug prior authorization. Web magellan rx management prior authorization request form fax completed form to: Magellan medicaid administration 11013 w broad street suite 500 glen allen, va 23060 fax: This form is made available for use by prescribers to initiate a. Reason authorization requires extension (provide detailed clinical information): Web prescription drug prior authorization (pa) request form fax to magellan pharmacy solutions:
Prior Authorization Form printable pdf download
Yes is this request for a yes continuation of therapy? If yes, what date was therapy started? Web prescription drug prior authorization (pa) request form fax to magellan pharmacy solutions: Request refills and track your specialty medications. Please fill out all applicable sections on all pages completely and legibly.

ads/responsive.txt Magellan Prior Authorization form Florida Fresh
Please refer to the dmas memo for more information. Ih.magellanrx.com patient information last name: Web date to which existing authorization should be extended: Starting november 1, 2023, all authorizations and registrations should be submitted to kepro. If yes, what date was therapy started?
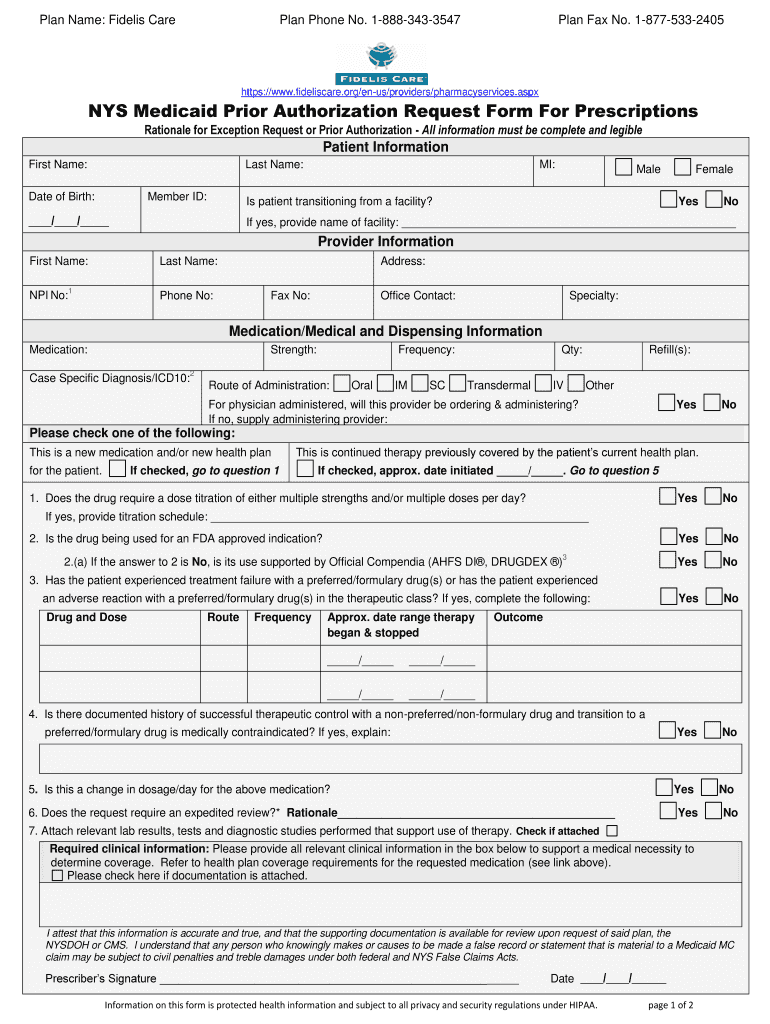
NY NYS Medicaid Prior Authorization Request Form For Prescriptions
Magellan medicaid administration 11013 w broad street suite 500 glen allen, va 23060 fax: Treatment authorization request form for 90837 mental health and substance use disorder. Attach any additional documentation that is important for the review (e.g., chart notes or lab data, to support the prior authorization). (nia) that provides ordering and rendering providers with instant access to prior authorization.

Aarp Radiology Prior Authorization Form Form Resume Examples
Instructions for retrospective review form; Please fill out all applicable sections on all pages completely and legibly. You simply file your claim and respond to any outreach calls from a magellan, should such occur. Web magellan rx management has partnered with covermymeds to offer electronic prior authorization (epa) services. 0.1 mg/kg subcutaneous (sc) qd or qod up to 6 mg.

Bcbs Prior Auth Form Texas Form Resume Examples pA8MQOk8Ra
You simply file your claim and respond to any outreach calls from a magellan, should such occur. Auxiliary forms (use as needed) Ih.magellanrx.com patient information last name: Web prescription drug prior authorization. Web if you are not the patient or the prescriber, you will need to submit a phi disclosure authorization form with this request which can be found at.
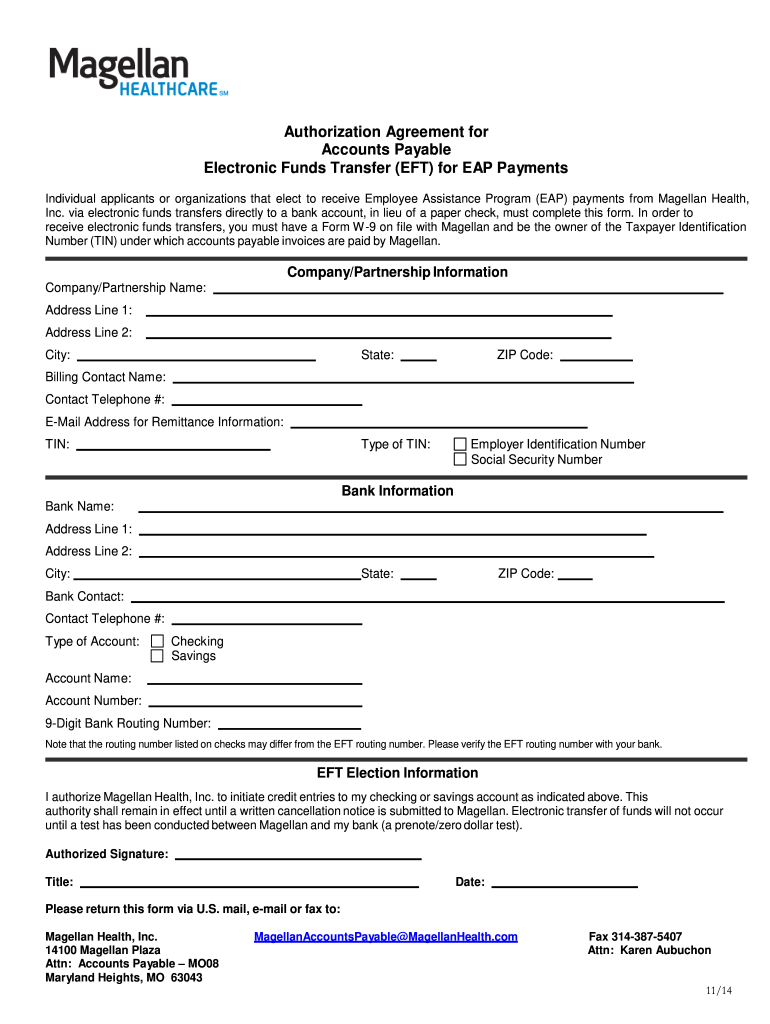
20142023 Form Magellan Healthcare Authorization Agreement for Accounts
Web date to which existing authorization should be extended: Yes is this request for a yes continuation of therapy? Ih.magellanrx.com patient information last name: Please fill out all applicable sections on all pages completely and legibly. Web prescription drug prior authorization form fax this form to:

ads/responsive.txt Magellan Prior Authorization form Florida Best Of
Auxiliary forms (use as needed) Web magellan rx management has partnered with covermymeds to offer electronic prior authorization (epa) services. Web prescription drug prior authorization form fax this form to: Web date to which existing authorization should be extended: Web magellan rx management prior authorization request form fax completed form to:

Proact Prior Authorization form Brilliant Arkansas Medicaid Magellan Rx
Select the appropriate magellan rx management form to get started. Ih.magellanrx.com patient information last name: Web request for psychological testing preauthorization form. If yes, what date was therapy started? Web date to which existing authorization should be extended:
Magellan Forms Fill Out and Sign Printable PDF Template signNow
If yes, what date was therapy started? Web request for psychological testing preauthorization form. Web prescription drug prior authorization form fax this form to: Select the appropriate magellan rx management form to get started. Request or access prior authorizations and view clinical guidelines.
Free Virginia Medicaid Prior Authorization Form PDF eForms
Web prior authorization request general pa form submit requests to: Please refer to the dmas memo for more information. Instructions for retrospective review form; Web request for psychological testing preauthorization form. Attach any additional documentation that is important for the review (e.g., chart notes or lab data, to support the prior authorization).
You Simply File Your Claim And Respond To Any Outreach Calls From A Magellan, Should Such Occur.
Web if you are not the patient or the prescriber, you will need to submit a phi disclosure authorization form with this request which can be found at the following link: Web magellan rx management prior authorization request form fax completed form to: Web prescription drug prior authorization. Web magellan rx management has partnered with covermymeds to offer electronic prior authorization (epa) services.
Request Refills And Track Your Specialty Medications.
Covermymeds is magellan rx management prior authorization forms’s preferred method for receiving epa requests. (nia) that provides ordering and rendering providers with instant access to prior authorization requests for specialty procedures. Web prior authorization request general pa form submit requests to: Ih.magellanrx.com patient information last name:
Web Magellan Rx Management Prior Authorization Request Form Fax Completed Form To:
Instructions for retrospective review form; Web prescription drug prior authorization (pa) request form fax to magellan pharmacy solutions: Magellan medicaid administration 11013 w broad street suite 500 glen allen, va 23060 fax: 0.1 mg/kg subcutaneous (sc) qd or qod up to 6 mg per day 1.
We’ve Designed The Documents In This Section To Support You In Your Quality Care Of Magellan Members.
Please fill out all questions completely and submit required clinical documentation where noted. Required medical information drug/product name: Whether submitting exam requests or checking the status of prior authorization requests, providers will. This form is made available for use by prescribers to initiate a.