Medical Redetermination Form Online
Medical Redetermination Form Online - Your continuing eligibility will be decided on the information. Through the mail or through the secure web portal, mycgs. Web if you need help completing a redetermination form you receive in the mail, call us or visit your local social security office. You may need to complete a renewal form. Note that data items are in groups of related information. During the cdr, we will also review your income ,. Your local county services office will either send a letter saying you qualify for another. Web to complete the redetermination process, the individual, guardian (if applicable) or approved representative must: Web a redetermination is the first level of an appeal. Date the service or item was received (mm/dd/yyyy).
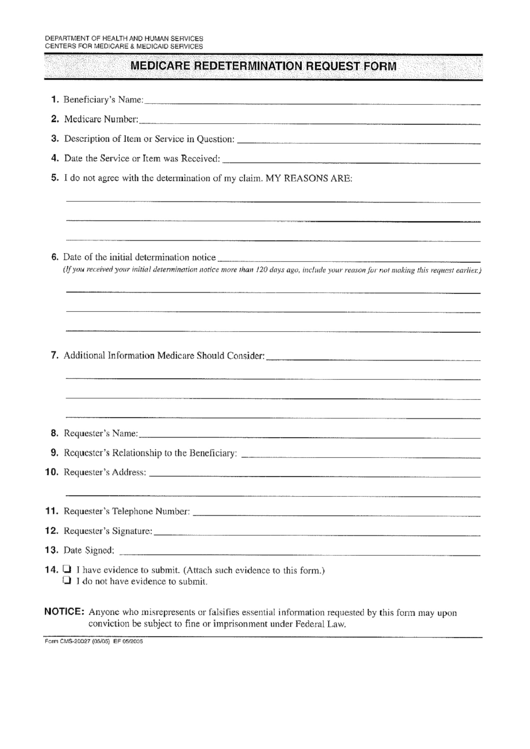
Your local county services office will either send a letter saying you qualify for another. Requesting an appeal (redetermination) if you. Note that data items are in groups of related information. Web please note that providers have two options to submit redetermination requests: An incomplete request is counted as a. Web medicare redetermination request form — 1st level of appeal beneficiary’s name (first, middle, last) medicare number item or service you wish to. Your continuing eligibility will be decided on the information. Complete the preprinted illinois medical, cash and snap. Ad digitize any existing form or easily create new forms to optimize your patient experience. Health insurance premium payment program.
Your local county services office will either send a letter saying you qualify for another. Web medicare redetermination request form — 1st level of appeal beneficiary’s name (first, middle, last) medicare number item or service you wish to. Health insurance premium program (hipp) application. Date the service or item was received (mm/dd/yyyy). Complete the preprinted illinois medical, cash and snap. Your continuing eligibility will be decided on the information. Web to complete the redetermination process, the individual, guardian (if applicable) or approved representative must: Beneficiary’s name (first, middle, last) medicare number. Web determination request form — 1st level of appeal. Complete fillable forms, register & subscribe now!

Example Medicare redetermination form Medicare Fee, Payment
Note that data items are in groups of related information. Beneficiary’s name (first, middle, last) medicare number. Web medicare redetermination request form — 1st level of appeal beneficiary’s name (first, middle, last) medicare number item or service you wish to. Complete the preprinted illinois medical, cash and snap. An incomplete request is counted as a.
Illinois Link Redetermination Online Fill Online, Printable, Fillable
Our staff will help you fill it out. Beneficiary’s name (first, middle, last) medicare number. Requesting an appeal (redetermination) if you. Web determination request form — 1st level of appeal. Web up to $40 cash back the ri dhs (rhode island department of human services) redetermination form is a document used by the department to reassess an individual's.
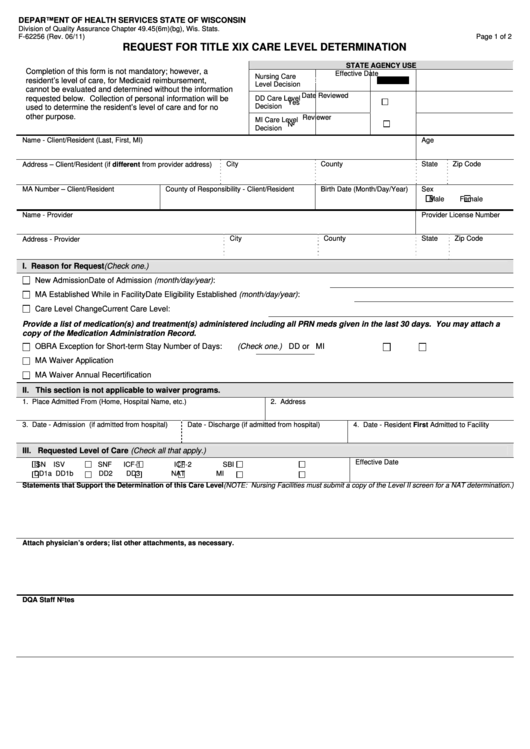
Form Cms20027 Medicare Redetermination Request Form, Form Cms20034
Note that data items are in groups of related information. Web a redetermination is the first level of an appeal. Web to complete the redetermination process, the individual, guardian (if applicable) or approved representative must: Web please note that providers have two options to submit redetermination requests: Your continuing eligibility will be decided on the information.
Form MC210 RV Download Printable PDF or Fill Online MediCal Annual
Beneficiary’s name (first, middle, last) medicare number. Note that data items are in groups of related information. For most members, coverage is renewed automatically. Our staff will help you fill it out. Web up to $40 cash back the ri dhs (rhode island department of human services) redetermination form is a document used by the department to reassess an individual's.

Ri Dhs Redetermination Form Fill Online, Printable, Fillable, Blank
Pdf fill and print forms. If you’re sent a renewal form, submit your. Date the service or item was received (mm/dd/yyyy). Web estate recovery forms. Note that data items are in groups of related information.
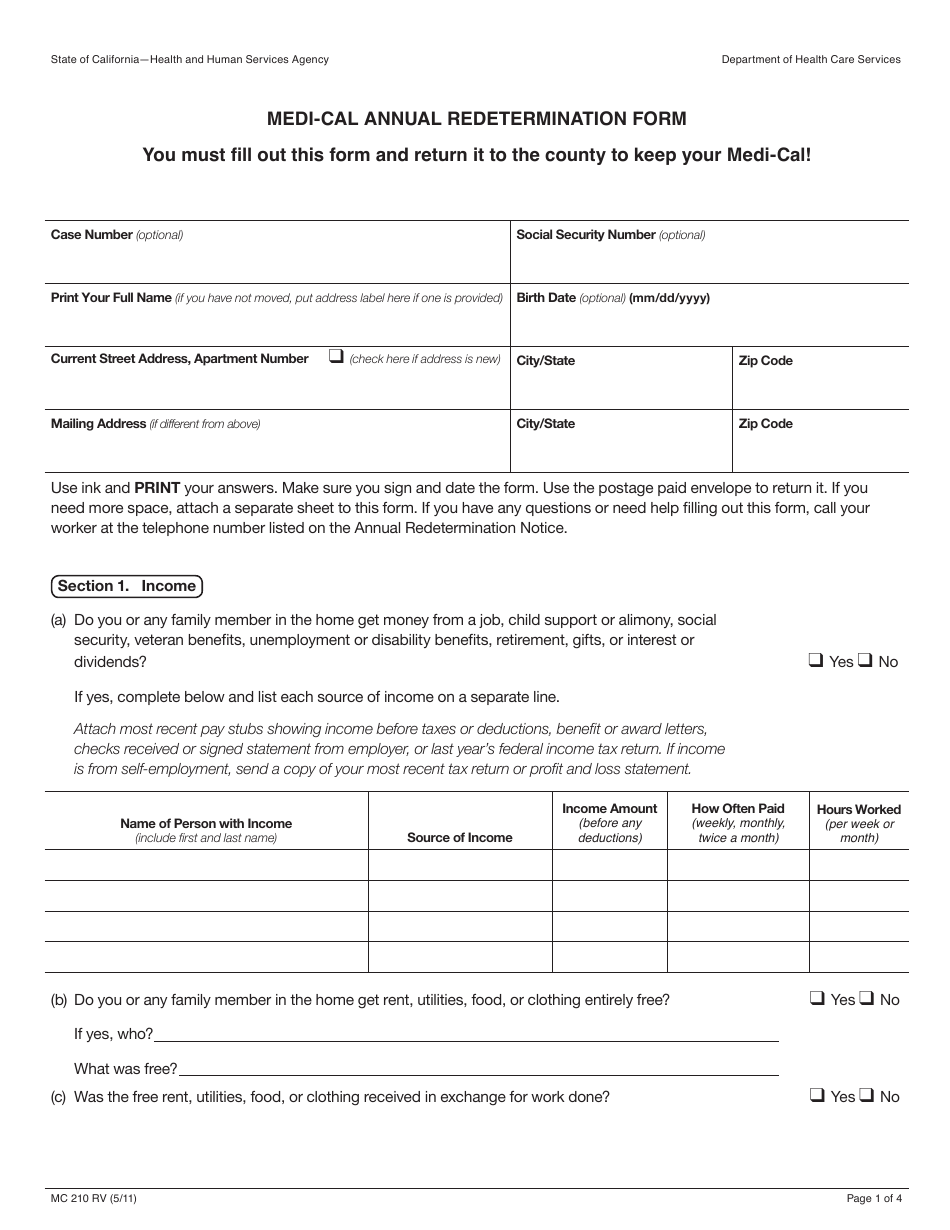
Form MC210 RV Download Fillable PDF or Fill Online MediCal Annual
Pdf fill and print forms. How to create an account. Beneficiary’s name (first, middle, last) medicare number. Note that data items are in groups of related information. Web paper form completion instructions are provided for each data item, which is indicated by a number.
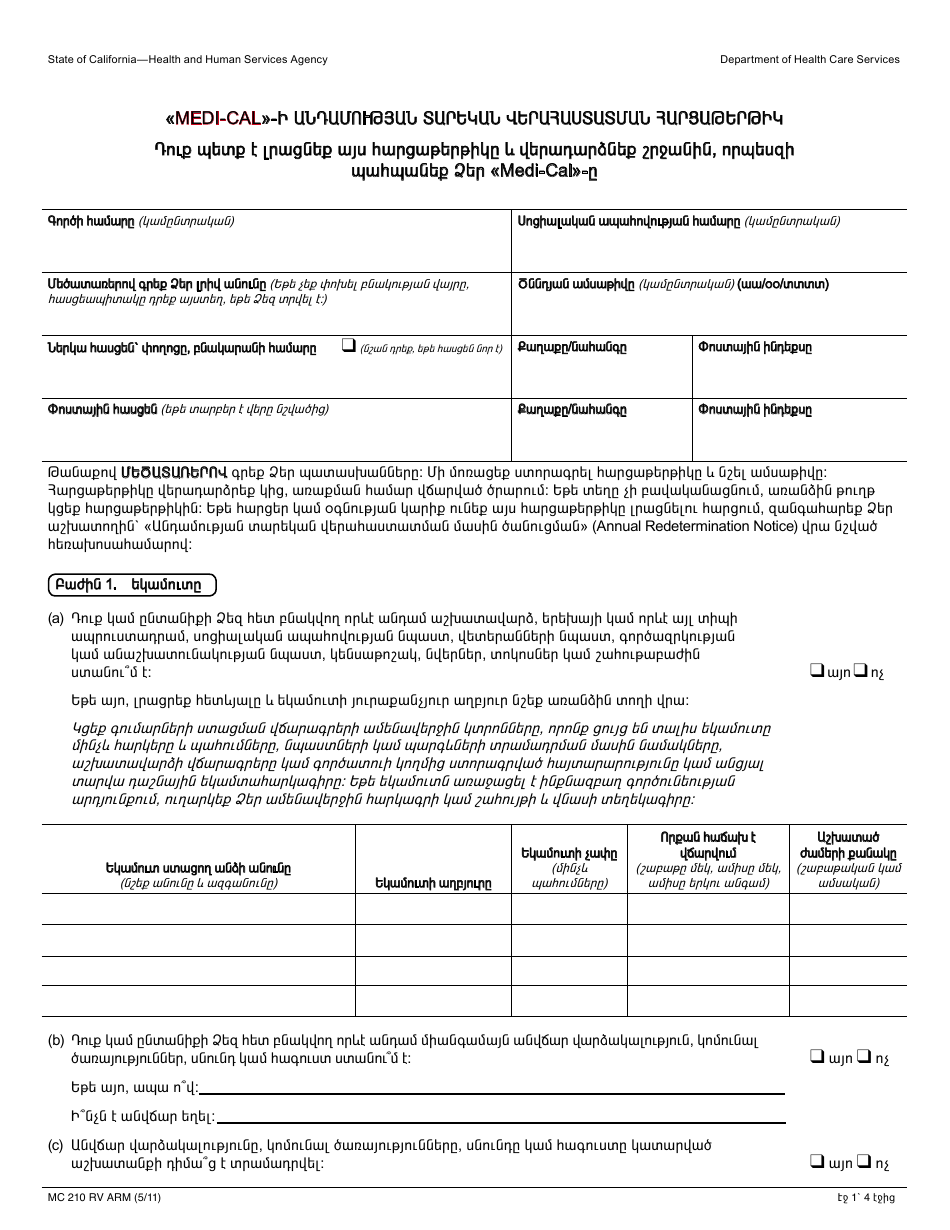
Form MC210 RV Download Printable PDF or Fill Online MediCal Annual
You will also learn what. Health insurance premium program (hipp) application. Complete the preprinted illinois medical, cash and snap. Our staff will help you fill it out. Your continuing eligibility will be decided on the information.
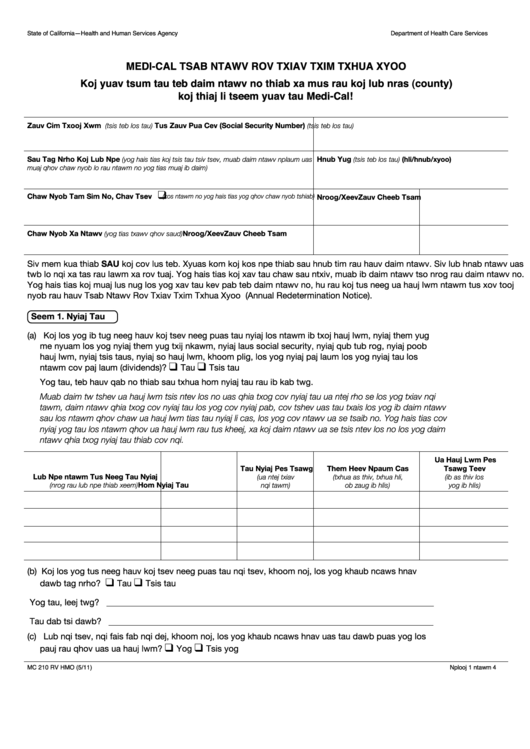
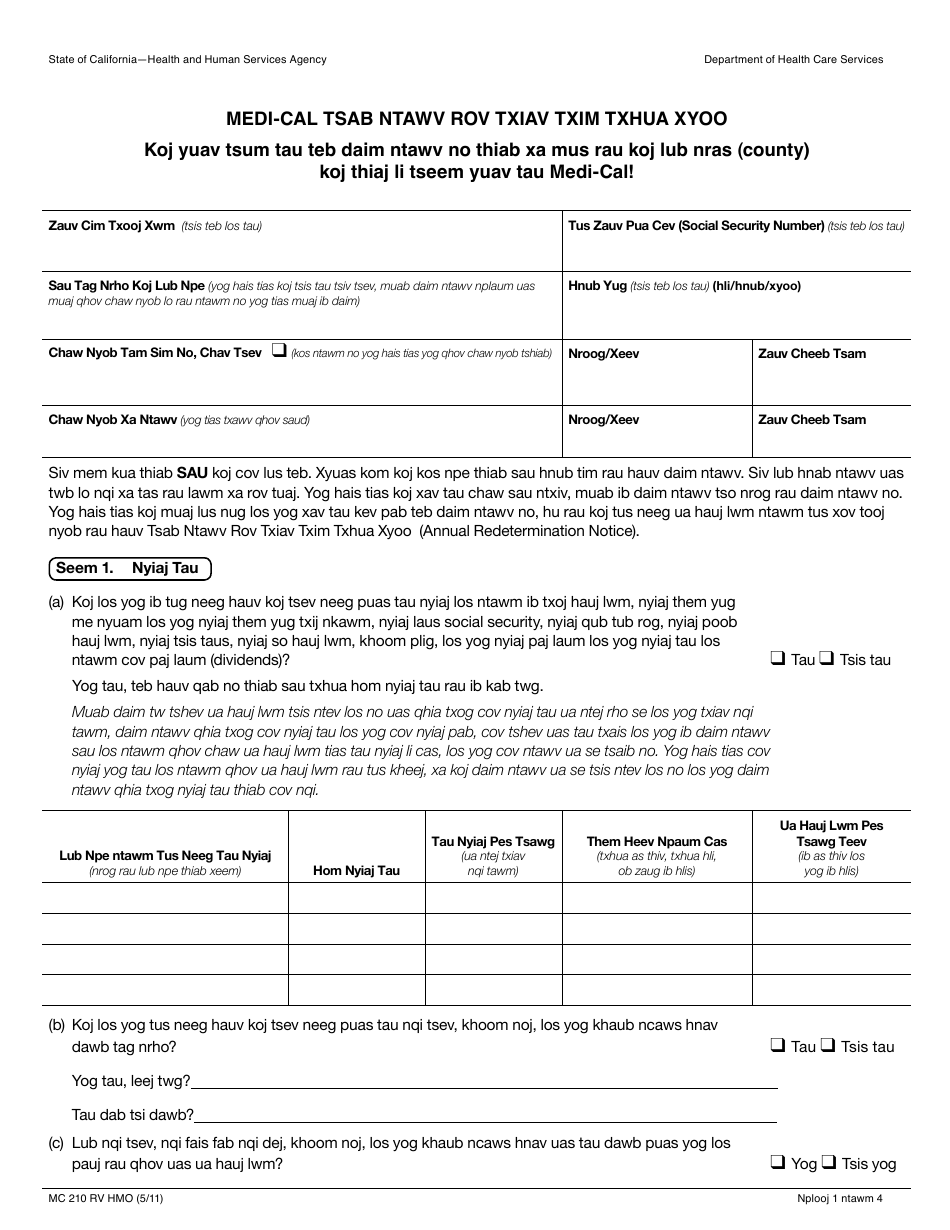
Form Mc 210 Rv MediCal Annual Redetermination Form (Hmong) printable
Web estate recovery forms. You may need to complete a renewal form. You will also learn what. An incomplete request is counted as a. Date the service or item was received (mm/dd/yyyy).
Top 10 Medicare Redetermination Form Templates free to download in PDF
Web medicare redetermination request form — 1st level of appeal beneficiary’s name (first, middle, last) medicare number item or service you wish to. Health insurance premium payment program. You may need to complete a renewal form. Complete fillable forms, register & subscribe now! Date the service or item was received (mm/dd/yyyy).

Medicare Redetermination Form 2020 2020 Fill and Sign Printable
Web to complete the redetermination process, the individual, guardian (if applicable) or approved representative must: Pdf fill and print forms. Our staff will help you fill it out. Health insurance premium program (hipp) application. Health insurance premium payment program.
Complete The Preprinted Illinois Medical, Cash And Snap.
Beneficiary’s name (first, middle, last) medicare number. Note that data items are in groups of related information. An incomplete request is counted as a. Web please note that providers have two options to submit redetermination requests:
Web Paper Form Completion Instructions Are Provided For Each Data Item, Which Is Indicated By A Number.
Web estate recovery forms. Your local county services office will either send a letter saying you qualify for another. Web up to $40 cash back the ri dhs (rhode island department of human services) redetermination form is a document used by the department to reassess an individual's. Web this review process is called your annual redetermination.
Pdf Fill And Print Forms.
Through the mail or through the secure web portal, mycgs. You may need to complete a renewal form. Complete fillable forms, register & subscribe now! Ad digitize any existing form or easily create new forms to optimize your patient experience.
Web If You Need Help Completing A Redetermination Form You Receive In The Mail, Call Us Or Visit Your Local Social Security Office.
Date the service or item was received (mm/dd/yyyy). During the cdr, we will also review your income ,. Requesting an appeal (redetermination) if you. Health insurance premium payment program.