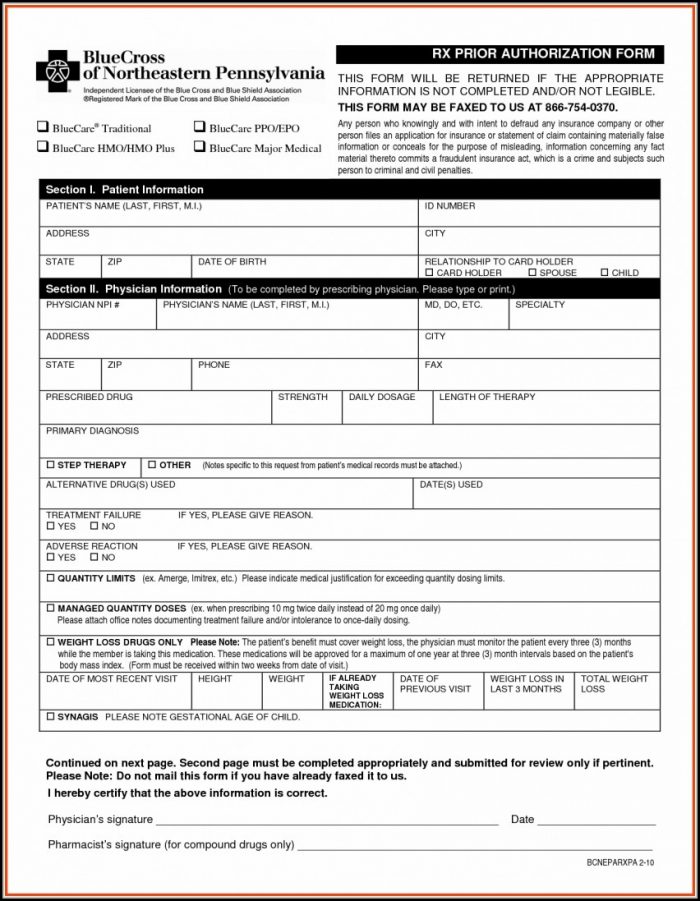
Metroplus Prior Authorization Form
Metroplus Prior Authorization Form - Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to. Web use our provider authorization grid for medical services below to determine what prior authorization requirements are applicable for various plans like. Web prior authorization request form phone: Hepatitis c prior authorization request form. You can also download it, export it or print it out. Easily fill out pdf blank, edit, and sign them. Web send metroplus prior authorization form via email, link, or fax. Web date form completed and faxed: Medicare speech therapy physical therapy occupational therapy fax: Save or instantly send your.
Easily fill out pdf blank, edit, and sign them. Web use our provider authorization grid for medical services below to determine what prior authorization requirements are applicable for various plans like. Web prior authorization request form fax: Physician administered drugs requiring step therapy effective 1/1/2023, select provider. Edit your m11q form metroplus online type text, add images,. Choose the form you require in the library of. Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to. Web modify, sign, and release metroplus authorization request form online. Metroplus health plan authorization request form, metroplus medicaid prior authorization form,. Web looking for metroplus prior authorization to fill?
Web use our provider authorization grid for medical services below to determine what prior authorization requirements are applicable for various plans like. Nope need to install software, just losfahren to dochub, and sign up directly and for free. Web prior authorization request form fax: Easily fill out pdf blank, edit, and sign them. Save or instantly send your. Medicare speech therapy physical therapy occupational therapy fax: Metroplus health plan authorization request form, metroplus medicaid prior authorization form,. Hepatitis c prior authorization request form. Save or instantly send your ready documents. Web modify, sign, and release metroplus authorization request form online.
Ach Payment Authorization Form Template Template 2 Resume Examples
Web metroplus health plan author: Stick to these simple actions to get metroplus authorization request form ready for sending: Web modify, sign, and release metroplus authorization request form online. Choose the form you require in the library of. Web it only takes a few minutes.

Metroplus Authorization Request Form
_____ *please attach the most recent clinical notes or supporting documentation* metroplus health plan pharmacy utilization management. Save or instantly send your. Web prior authorization request form phone: Metroplus health plan authorization request form, metroplus medicaid prior authorization form,. Cocodoc is the best place for you to go, offering you a free and modifiable version of metroplus prior authorization as.
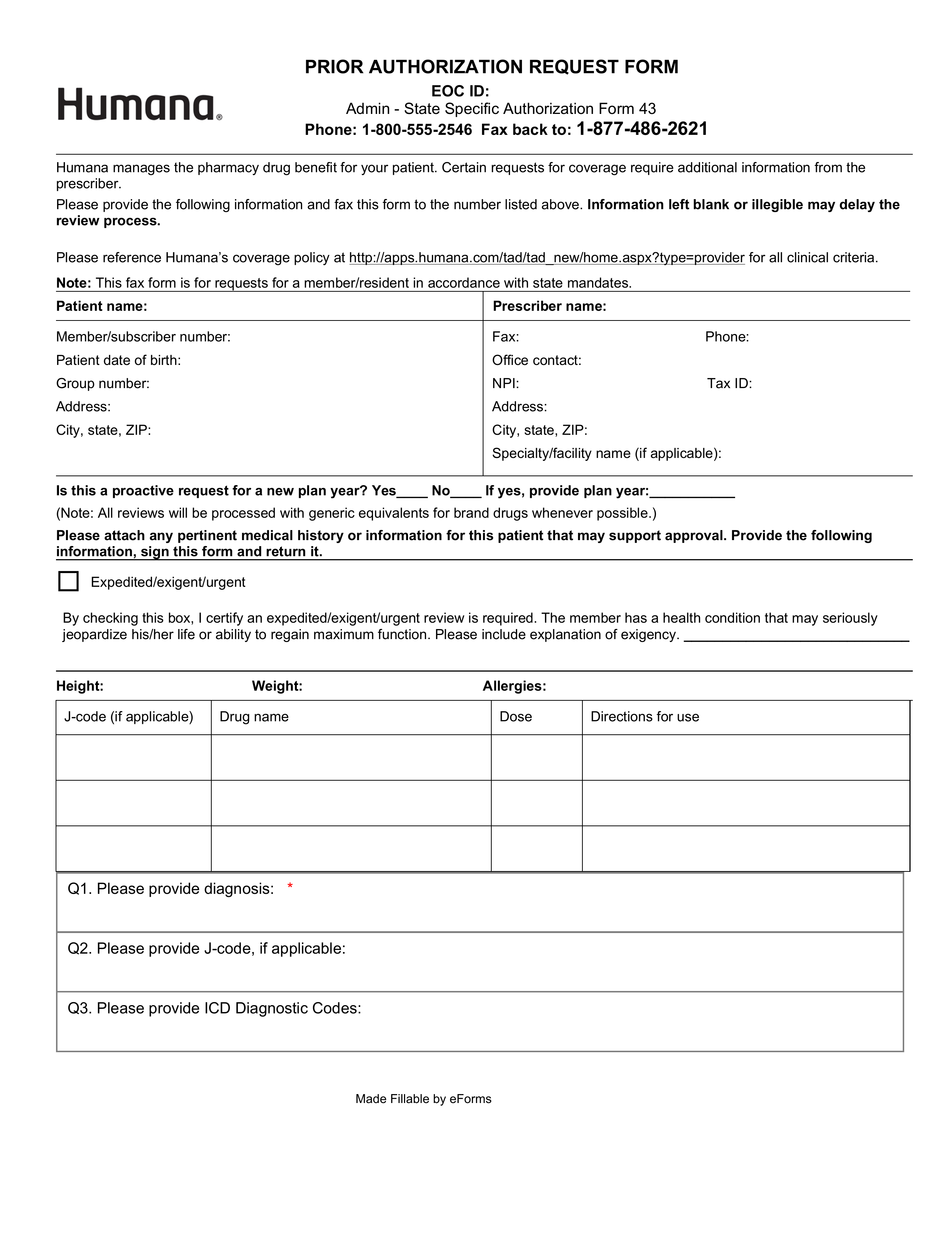
Free Humana Prior (Rx) Authorization Form PDF eForms
Cocodoc is the best place for you to go, offering you a free and modifiable version of metroplus prior authorization as you ask. Web it only takes a few minutes. Hepatitis c prior authorization request form. Nope need to install software, just losfahren to dochub, and sign up directly and for free. Physician administered drugs requiring step therapy effective 1/1/2023,.
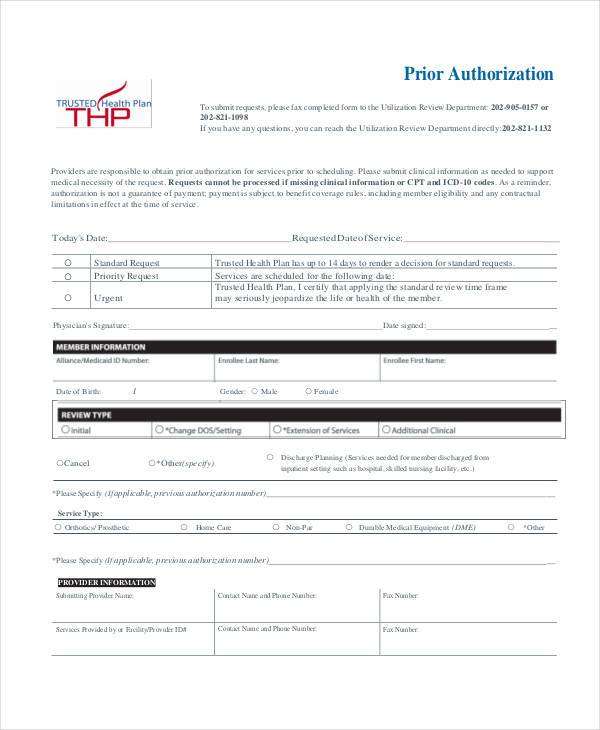
Medicare Hospital Stay 3 Days Medicare Prescription Prior
Physician administered drugs requiring step therapy effective 1/1/2023, select provider. Web modify, sign, and release metroplus authorization request form online. Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to. Edit your m11q form metroplus online type text, add images,. Easily fill out pdf blank, edit, and.

Covermymeds Prior Authorization Form Pdf Form Resume Examples
Web complete metroplus prior authorization form online with us legal forms. Please ensure completion of this form in its entirety and attach required. Choose the form you require in the library of. Save or instantly send your. Metroplus health plan pharmacy utilization management department 50 water street 7th floor, new york, ny.
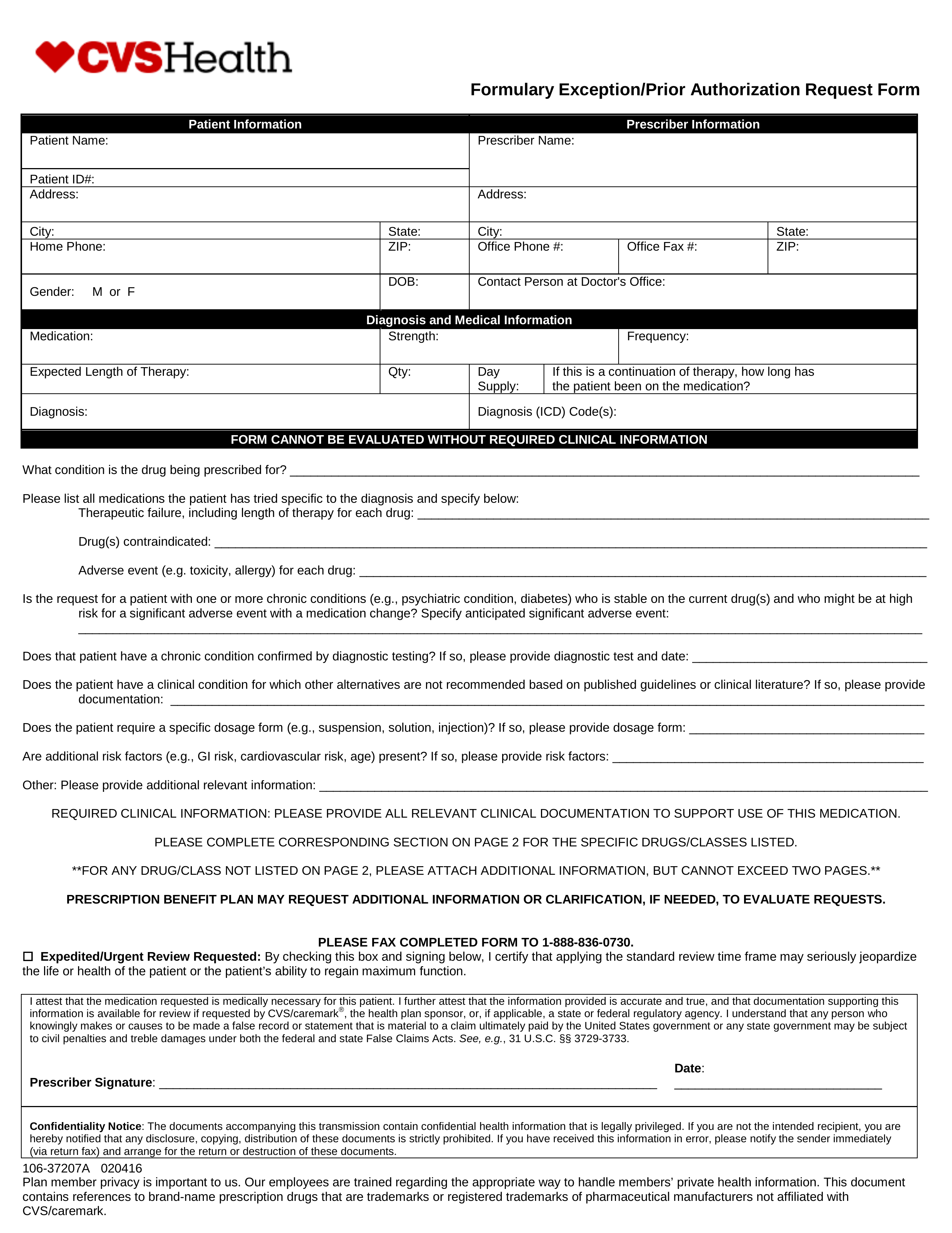
Free CVS/Caremark Prior (Rx) Authorization Form PDF eForms
Web looking for metroplus prior authorization to fill? Easily fill out pdf blank, edit, and sign them. Web date form completed and faxed: Web the metroplus prior authorization form can be found here. Web modify, sign, and release metroplus authorization request form online.
FREE 8+ Sample Prior Authorization Forms in PDF MS Word
Physician administered drugs requiring step therapy effective 1/1/2023, select provider. Web modify, sign, and release metroplus authorization request form online. Save or instantly send your. Medicare speech therapy physical therapy occupational therapy fax: Cocodoc is the best place for you to go, offering you a free and modifiable version of metroplus prior authorization as you ask.

Medicare Generation Rx Prior Authorization Form Form Resume
Physician administered drugs requiring step therapy effective 1/1/2023, select provider. Please ensure completion of this form in its entirety and attach required. Web submission of request form required for: Save or instantly send your. Metroplus health plan authorization request form, metroplus medicaid prior authorization form,.
MetroPlus Health Plan S. Hasan Physician PC
Web send metroplus prior authorization form via email, link, or fax. Web it only takes a few minutes. Web use our provider authorization grid for medical services below to determine what prior authorization requirements are applicable for various plans like. Web prior authorization request form phone: Save or instantly send your ready documents.
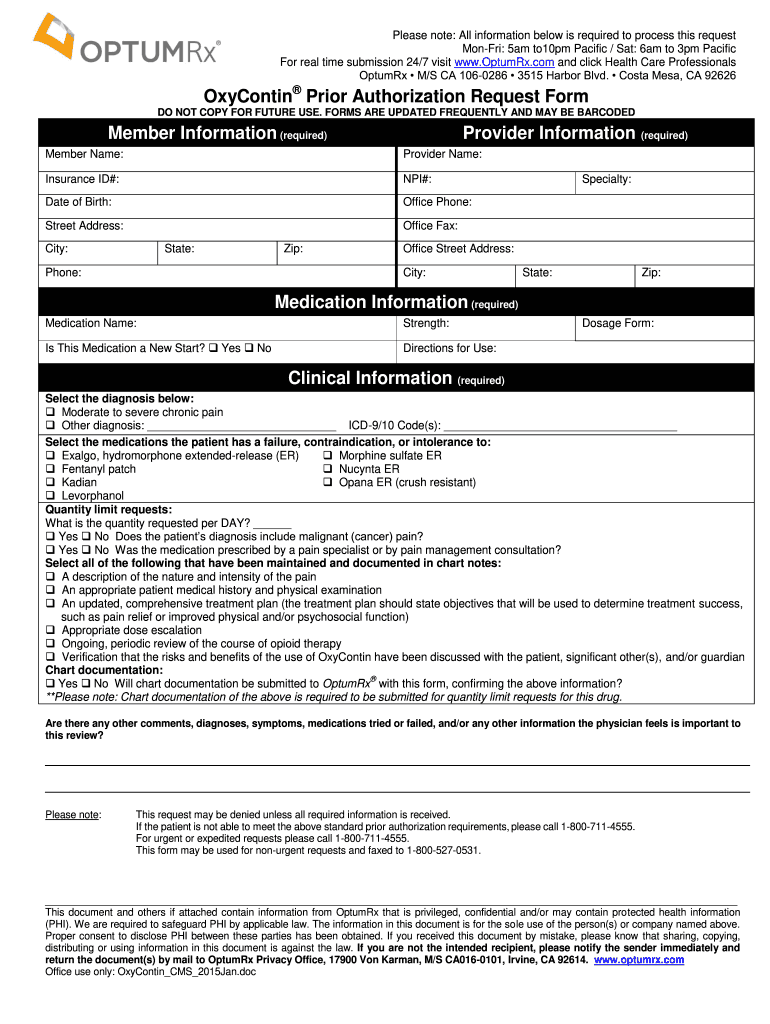
Optum rx oxycontin pa form Fill Out and Sign Printable PDF Template
Choose the form you require in the library of. Web it only takes a few minutes. Medicare speech therapy physical therapy occupational therapy fax: Web prior authorization request form fax: Web prior authorization request form phone:
You Can Also Download It, Export It Or Print It Out.
Easily fill out pdf blank, edit, and sign them. Save or instantly send your. Save or instantly send your ready documents. Web it only takes a few minutes.
Web Use Our Provider Authorization Grid For Medical Services Below To Determine What Prior Authorization Requirements Are Applicable For Various Plans Like.
Metroplus health plan pharmacy utilization management department 50 water street 7th floor, new york, ny. Edit your m11q form metroplus online type text, add images,. Choose the form you require in the library of. Cocodoc is the best place for you to go, offering you a free and modifiable version of metroplus prior authorization as you ask.
Hepatitis C Prior Authorization Request Form.
_____ *please attach the most recent clinical notes or supporting documentation* metroplus health plan pharmacy utilization management. Web prior authorization request form fax: Web metroplus health plan author: Web send metroplus prior authorization form via email, link, or fax.
Web The Metroplus Prior Authorization Form Can Be Found Here.
Easily fill out pdf blank, edit, and sign them. Web i general authorization request form please fax this form along with supporting clinical documentation to the appropriate fax number below (corresponding to. Web prior authorization request form phone: Web submission of request form required for: