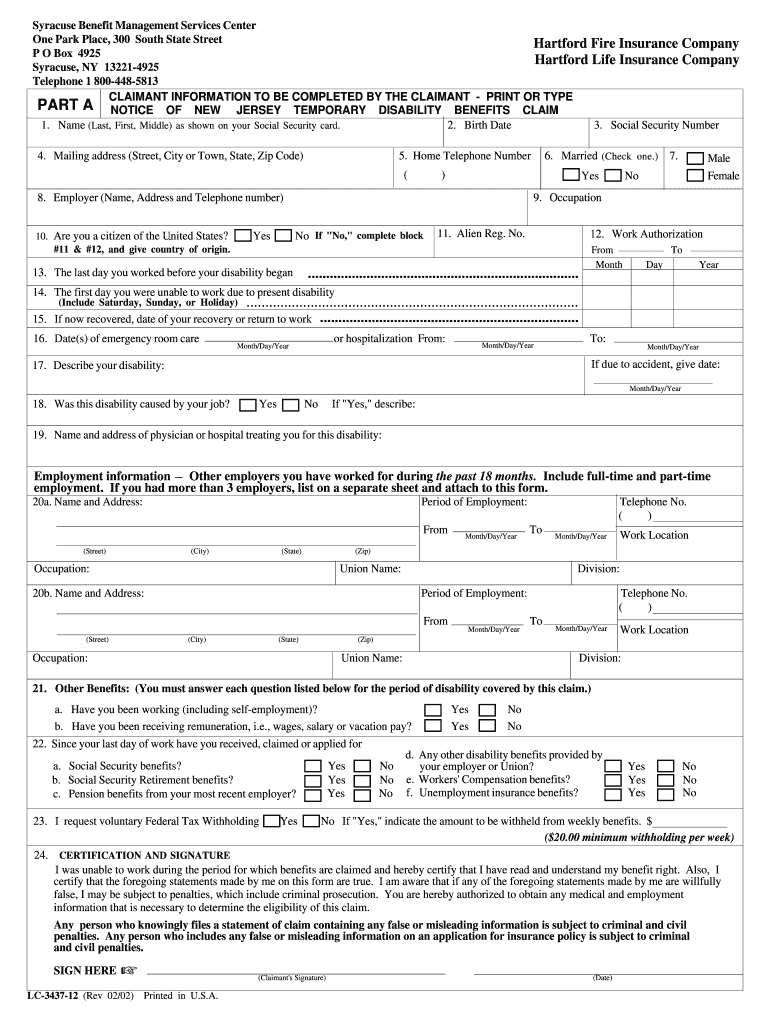
New York State Disability Claim Form
New York State Disability Claim Form - If you are using this form because you became disabled while employed or. The board recommends using the latest version of adobe reader which is available as a free download from adobe's website. Medical care is the responsibility of the employee and is not paid for by the employer or insurance carrier. Web the disability benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). Web disability benefits forms employees forms completing forms if you require assistance with completing these forms, please contact us. Web enter your information for your claim. In order for your claim to be processed, parts a and b must be completed. For approved claims, disability benefits begin on the eighth day of disability. Forms are in pdf format. Submit your online application with the federal social security administration.
Disability benefits are equal to 50 percent of the employee's average weekly wage for the last eight weeks worked, with a maximum benefit of $170 per week (wcl §204). Do not date and file this form prior to your first date of disability. Follow instructions to complete/submit the form, which includes a section your health care provider must complete. Web the disability benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). Forms are in pdf format. Web your completed claim should be mailed to: Web disability benefits forms employees forms completing forms if you require assistance with completing these forms, please contact us. Web the disability and paid family leave benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). In order for your claim to be processed, parts a and b must be completed. Submit your online application with the federal social security administration.
Submit your online application with the federal social security administration. Web disability benefits forms employees forms completing forms if you require assistance with completing these forms, please contact us. If you do not receive a response within 45 days or if you have questions about your disability benefits claim,. Web the disability benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). If you are using this form because you became disabled while employed or. Follow instructions to complete/submit the form, which includes a section your health care provider must complete. Web the disability and paid family leave benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). For approved claims, disability benefits begin on the eighth day of disability. Medical care is the responsibility of the employee and is not paid for by the employer or insurance carrier. Disability benefits are equal to 50 percent of the employee's average weekly wage for the last eight weeks worked, with a maximum benefit of $170 per week (wcl §204).
Nj State Disability Forms Printable Fill Out and Sign Printable PDF
If you are using this form because you became disabled while employed or. Web the disability benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). If you do not receive a response within.
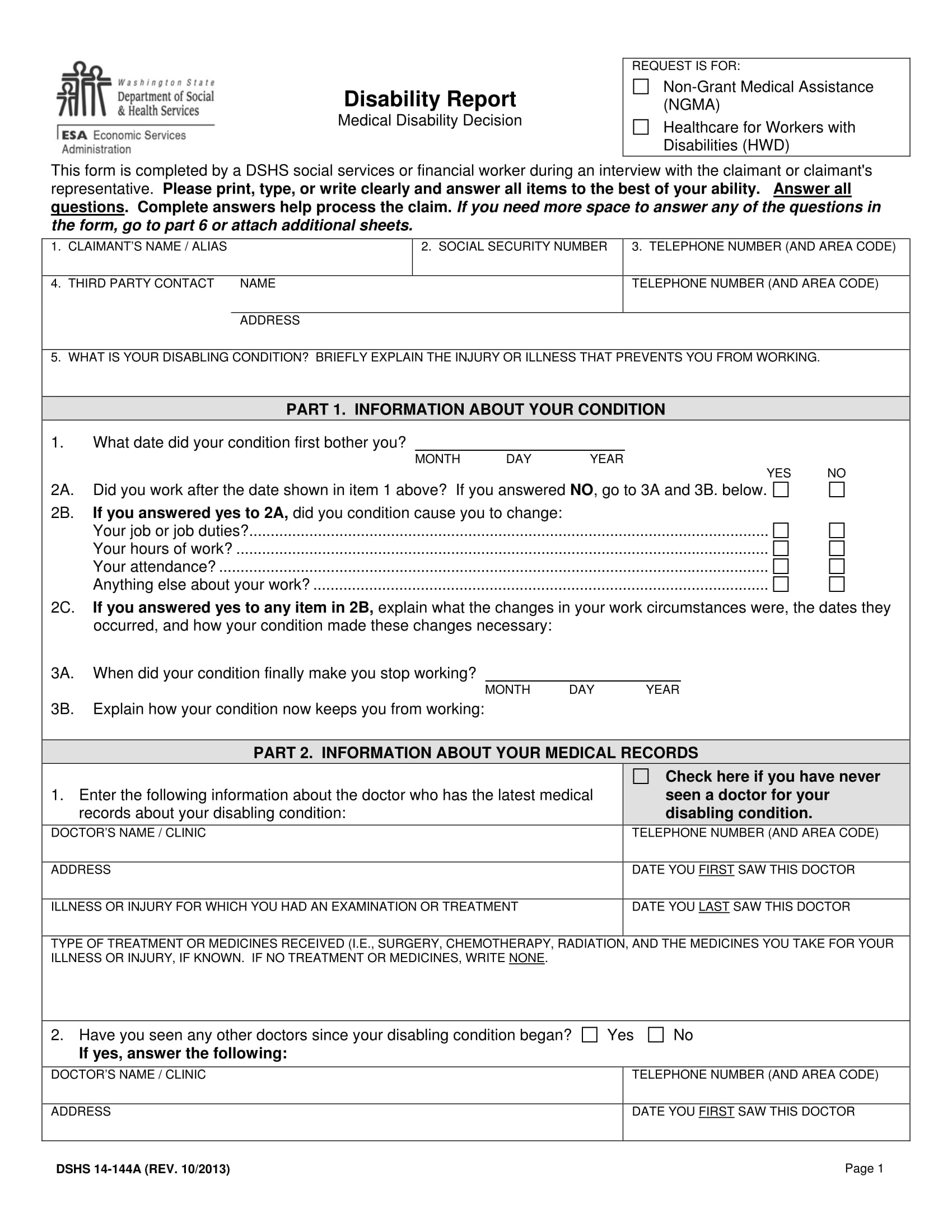
FREE 14+ Disability Report Forms in PDF
The board recommends using the latest version of adobe reader which is available as a free download from adobe's website. Web the disability benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). Do.

Va Disability Claim Form 21 526 Form Resume Examples q78QqXRJ8g
Web the disability benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). Medical care is the responsibility of the employee and is not paid for by the employer or insurance carrier. Web disability.

2021 Form NY Standard Insurance Company SNY 9457 Fill Online, Printable
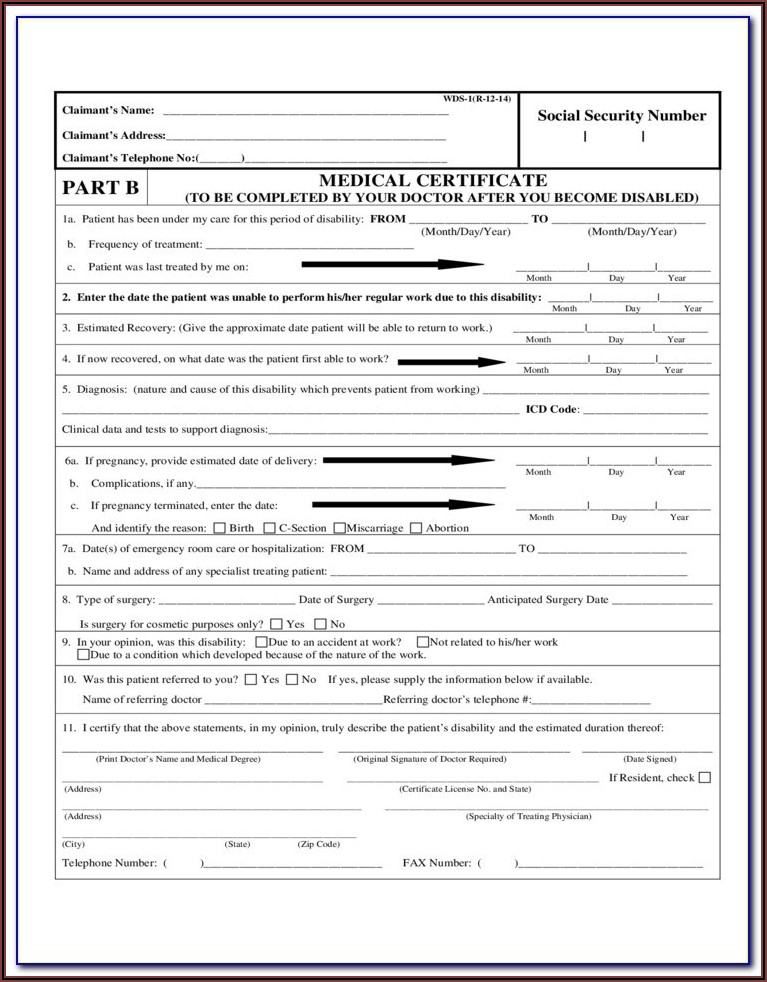
Follow instructions to complete/submit the form, which includes a section your health care provider must complete. Medical care is the responsibility of the employee and is not paid for by the employer or insurance carrier. Disability benefits are equal to 50 percent of the employee's average weekly wage for the last eight weeks worked, with a maximum benefit of $170.
California State Disability Claim Form De 2501 Form Resume Examples
Web enter your information for your claim. Web the disability benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). Web your completed claim should be mailed to: If you do not receive a.

New york state disability insurance insurance
Web disability benefits forms employees forms completing forms if you require assistance with completing these forms, please contact us. Medical care is the responsibility of the employee and is not paid for by the employer or insurance carrier. Disability benefits are equal to 50 percent of the employee's average weekly wage for the last eight weeks worked, with a maximum.
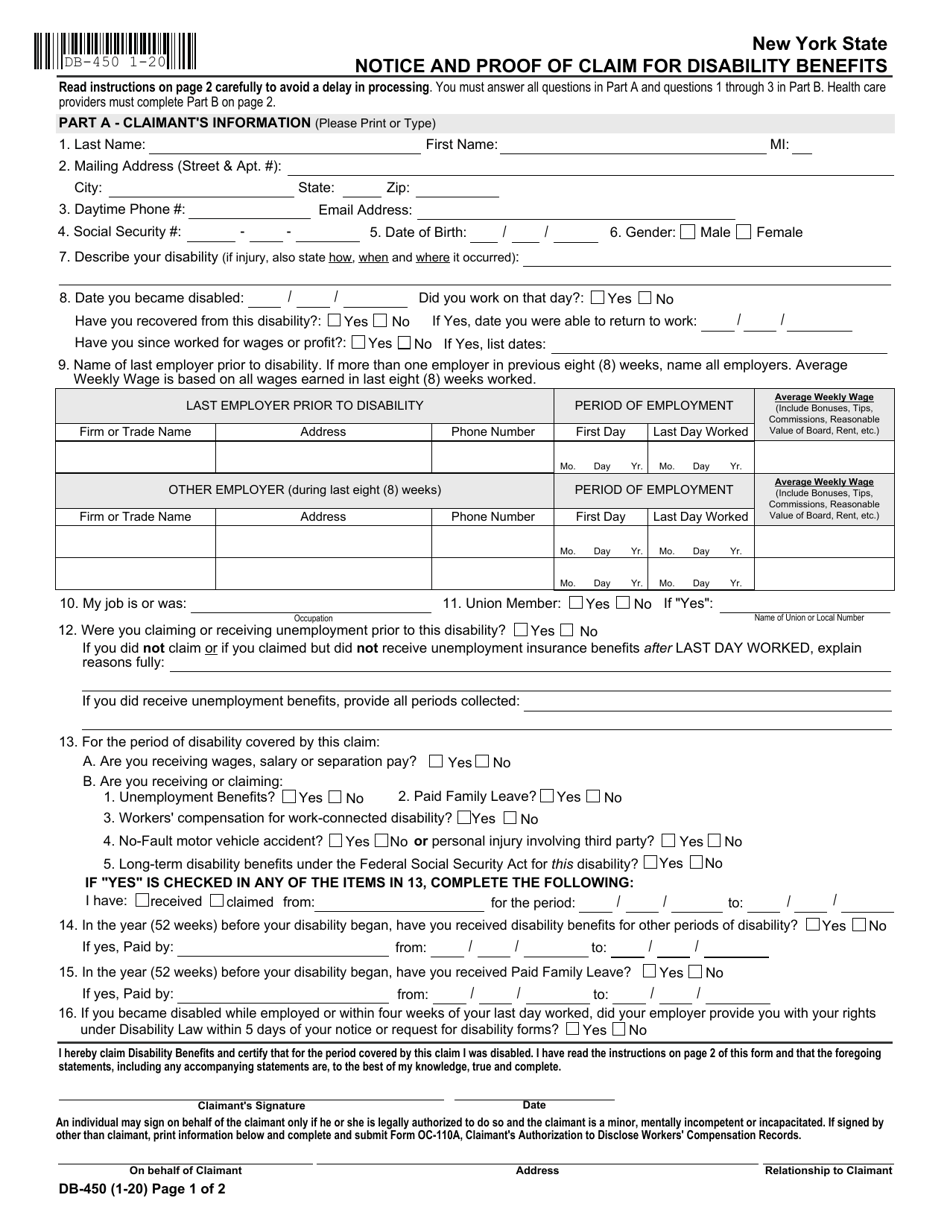
Form DB450 Fill Out, Sign Online and Download Fillable PDF, New York
A disability analyst from the nys division of disability determinations will review your case and determine whether or not you are disabled according to federal guidelines. Web your completed claim should be mailed to: Do not date and file this form prior to your first date of disability. If you are using this form because you became disabled while employed.

2004 Form NY DB450 Fill Online, Printable, Fillable, Blank pdfFiller
A disability analyst from the nys division of disability determinations will review your case and determine whether or not you are disabled according to federal guidelines. Web enter your information for your claim. The board recommends using the latest version of adobe reader which is available as a free download from adobe's website. Submit your online application with the federal.

Ca Ssi Disability Forms Universal Network
The board recommends using the latest version of adobe reader which is available as a free download from adobe's website. Web the disability and paid family leave benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of.
Fillable State Form 42070 Application For Disability Plate Or Parking
The board recommends using the latest version of adobe reader which is available as a free download from adobe's website. Web enter your information for your claim. For approved claims, disability benefits begin on the eighth day of disability. Web your completed claim should be mailed to: Web the disability benefits law (article 9 of the wcl) provides weekly cash.
The Board Recommends Using The Latest Version Of Adobe Reader Which Is Available As A Free Download From Adobe's Website.
Web the disability and paid family leave benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204). A disability analyst from the nys division of disability determinations will review your case and determine whether or not you are disabled according to federal guidelines. In order for your claim to be processed, parts a and b must be completed. Web the disability benefits law (article 9 of the wcl) provides weekly cash benefits to replace, in part, wages lost due to injuries or illnesses that do not arise out of or in the course of employment (wcl §204).
If You Do Not Receive A Response Within 45 Days Or If You Have Questions About Your Disability Benefits Claim,.
Follow instructions to complete/submit the form, which includes a section your health care provider must complete. Web enter your information for your claim. Submit your online application with the federal social security administration. Forms are in pdf format.
Do Not Date And File This Form Prior To Your First Date Of Disability.
Medical care is the responsibility of the employee and is not paid for by the employer or insurance carrier. For approved claims, disability benefits begin on the eighth day of disability. Web your completed claim should be mailed to: If you are using this form because you became disabled while employed or.
Disability Benefits Are Equal To 50 Percent Of The Employee's Average Weekly Wage For The Last Eight Weeks Worked, With A Maximum Benefit Of $170 Per Week (Wcl §204).
Web disability benefits forms employees forms completing forms if you require assistance with completing these forms, please contact us.