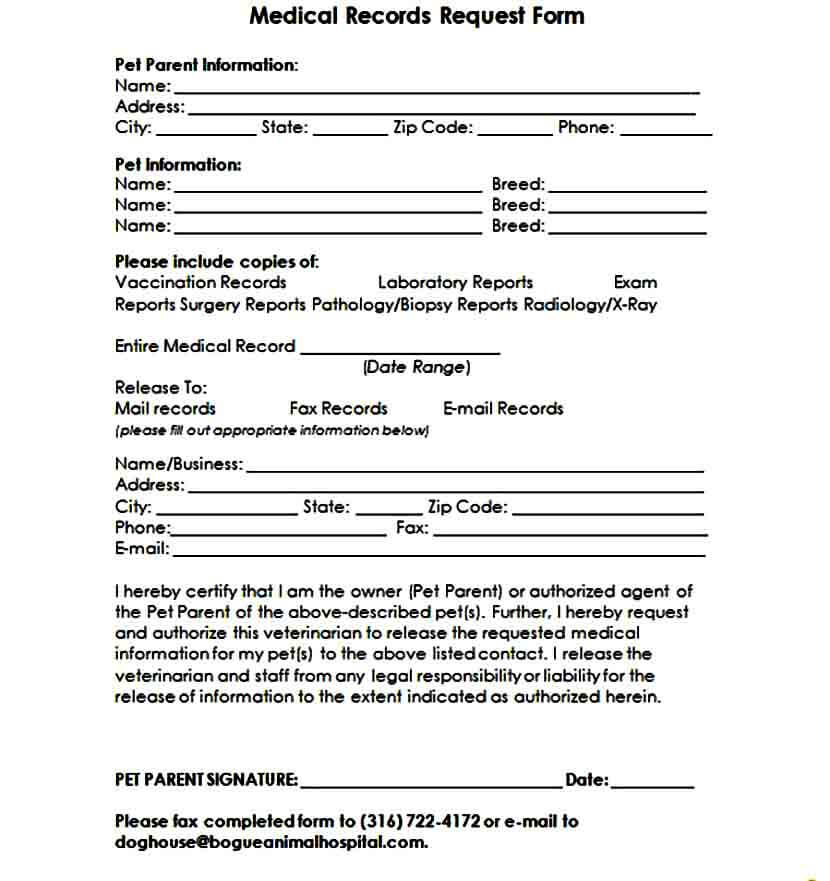
Sample Medical Records Request Form
Sample Medical Records Request Form - Web in order to pass on your medical information you must authorize it by utilizing a medical records release form. Request your medical records free of charge via myportfolio. I, ________, hereby authorize the following individual at the following address: This may include a hospital, clinic, doctor’s office, or other healthcare facility. After entering a few key pieces of information, your records can be released to you through myportfolio at no charge. Child medical records request form; Web i request copies of the following [or all] health records related to my treatment. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Make & save a customized medical records request with rocket lawyer. Web request a copy of your medical records.
(name of patient) patient information: This may include a hospital, clinic, doctor’s office, or other healthcare facility. Request your medical records free of charge via myportfolio. Medical records release form 1 document. Test results, consultations with specialists; Web sample military medical records request form archives.gov details file format pdf size: Web record and track key medical information, like medications, surgical procedures, illnesses, and vaccinations with this medical history form template. Printable medical record release form southshoreurology.com Here is a sample medical records authorization form you can complete to help your attorney or personal representative request and obtain your health care records. Medical release form 71 documents.
Choose this template start by clicking on fill out the template 2. Any patient that has various requests related to medical providers, medical facilities, physicians, specialists, or medical services will need this authorization request. Web the medical history record pdf template means to provide the doctor patient's health history. Complete the document answer a few questions and your document is created automatically. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Web medical request form sample; Medical release form 71 documents. I, ________, hereby authorize the following individual at the following address: Printable medical record release form southshoreurology.com 55 kb download the form is used when an authorized person or organization is giving permission to any other organization to access the medical records of any specific disease of an individual to use for the further treatment.
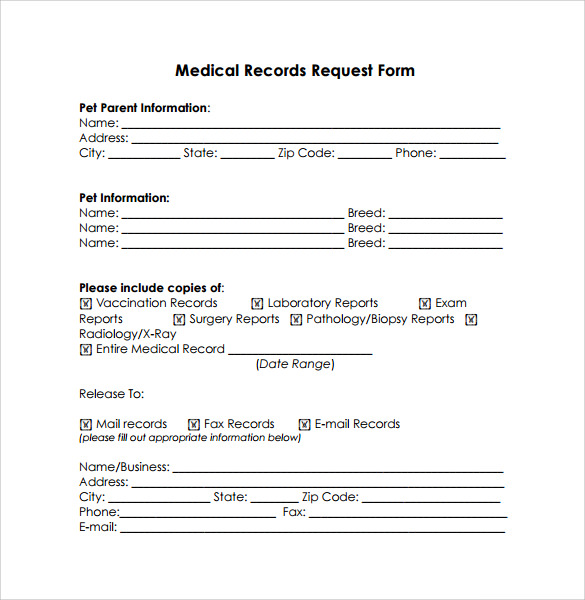
FREE 6+ Sample Medical Record Request Forms in PDF
Web the medical history record pdf template means to provide the doctor patient's health history. Child medical records request form; Medical consent form 36 documents. Medical history form you provided; Authorization request form who needs this?
Sample Medical Record Request Form Template Addictionary Medical
Medical history form 76 documents. You will receive it in word and pdf formats. Web record and track key medical information, like medications, surgical procedures, illnesses, and vaccinations with this medical history form template. Web medical records request letter [your name] [address] [city, state, zip] [date of letter] [name of care provider or facility] [address] [city, state, zip] dear [recipient's.
Sample Medical Records Request Form Mous Syusa
You’ll find space to document medication dosage and frequency, chronic illnesses, and prior vaccination dates, so no detail is forgotten or overlooked. 55 kb download the form is used when an authorized person or organization is giving permission to any other organization to access the medical records of any specific disease of an individual to use for the further treatment..
Medical Records Request Form in Word and Pdf formats
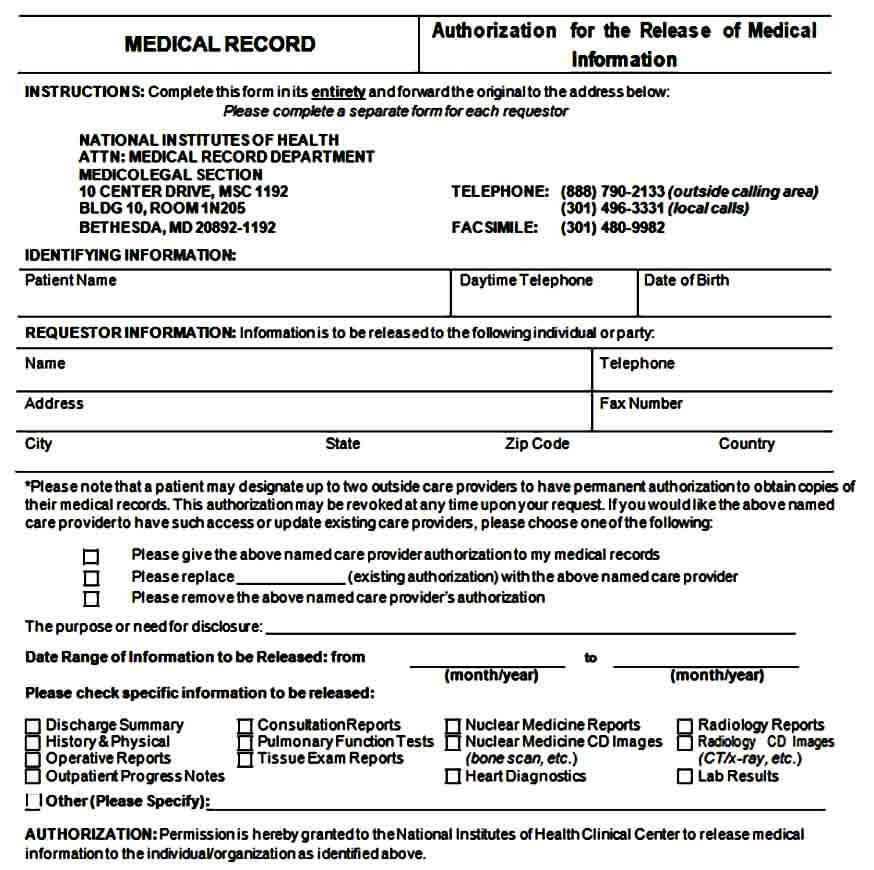
Medical clearance form 14 documents. Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Web sample military medical records request form archives.gov details file format pdf size: Web medical claim form 9 documents. ________ ________ to release, disclose, and deliver the medical information described.
Sample Medical Records Release Form Mous Syusa
Medical power of attorney form 6 documents. Medical history form you provided; (name of patient) patient information: Identify the recipient begin the letter by addressing the healthcare provider or medical facility that has custody of the medical records. Web medical request form sample;

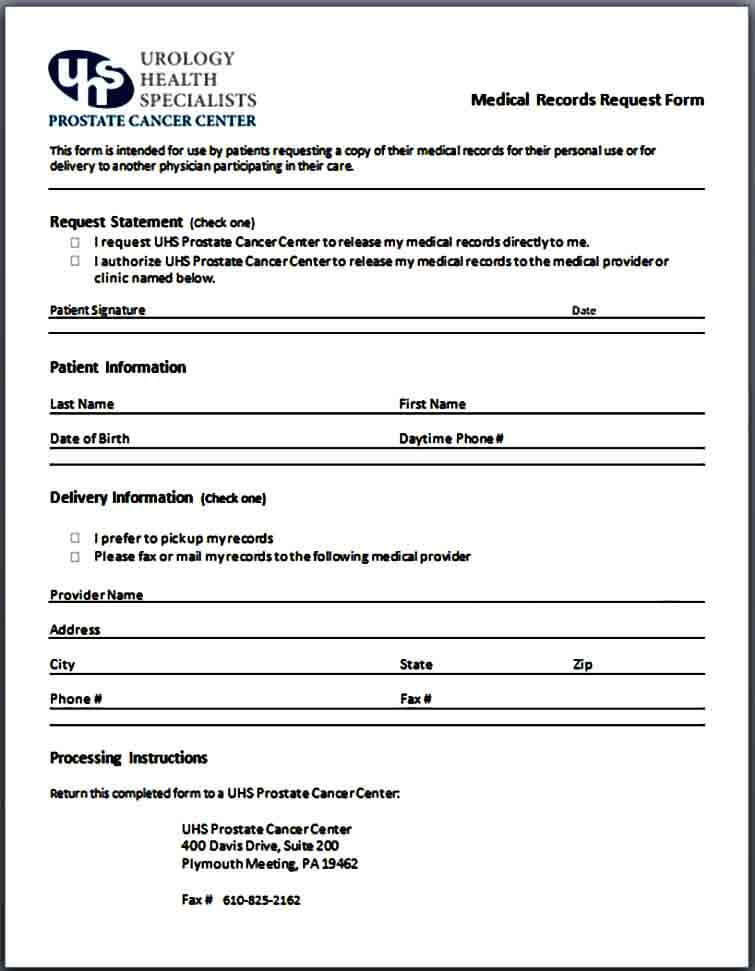
FREE 12+ Medical Records Request Forms in PDF Word
Printable medical record release form southshoreurology.com Medical release form 71 documents. Medical waiver form 11 documents. After entering a few key pieces of information, your records can be released to you through myportfolio at no charge. Here is a sample medical records authorization form you can complete to help your attorney or personal representative request and obtain your health care.
Sample Medical Records Release Form Mous Syusa
26 kb download hipaa medical records request form washingtonendocrineclinic.com details file format pdf size: Web medical claim form 9 documents. Medical power of attorney form 6 documents. Medical waiver form 11 documents. Authorization request form who needs this?
11+ Medical Records Release Forms Samples, Examples & Format Sample
Web to request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Test results, consultations with specialists; By using this medical history record pdf template you can collect the patient's data such as personal information. 20+ sample medical release forms sample forms. Web sample medical records request.
Sample Medical Records Request Form Mous Syusa
I, ________, hereby authorize the following individual at the following address: Web accessing and obtaining your medical records is a requirement under 45 cfr 164.524 which requires that any request made to access or transfer medical records must be completed within 30 days, or a letter must be sent to the requestor stating why the records are delayed. Web 7+.
Sample Medical Records Request Form Mous Syusa
Complete the document answer a few questions and your document is created automatically. This may include a hospital, clinic, doctor’s office, or other healthcare facility. (name of patient) patient information: Web if you are requesting your medical records for personal use, you might write: Web i request copies of the following [or all] health records related to my treatment.
With The Help Of The Medical History Record Pdf Template, The Doctor Will Be Able To Ensure The Patient's Better Care And Treatment.
Medical records release forms are forms that give a set of permissions to people in certain situations, to allow a clinic, hospital or medical professional to release medical records. Temporary medical exemption request form. (name of patient) patient information: Web i request copies of the following [or all] health records related to my treatment.
Request Your Medical Records Free Of Charge Via Myportfolio.
Medical history form you provided; 20+ sample medical release forms sample forms. 1 mb download generic medical records request form in pdf texaschildrens.org details file format pdf size: ________ ________ to release, disclose, and deliver the medical information described below to.
Web Medical Records Request Letter [Your Name] [Address] [City, State, Zip] [Date Of Letter] [Name Of Care Provider Or Facility] [Address] [City, State, Zip] Dear [Recipient's Name], I Am Writing You To Request Copies Of My Medical Records.
Web accessing and obtaining your medical records is a requirement under 45 cfr 164.524 which requires that any request made to access or transfer medical records must be completed within 30 days, or a letter must be sent to the requestor stating why the records are delayed. Patient medical payment request form; Any patient that has various requests related to medical providers, medical facilities, physicians, specialists, or medical services will need this authorization request. Complete the document answer a few questions and your document is created automatically.
This May Include A Hospital, Clinic, Doctor’s Office, Or Other Healthcare Facility.
Here is a sample medical records authorization form you can complete to help your attorney or personal representative request and obtain your health care records. Make & save a customized medical records request with rocket lawyer. Printable medical record release form southshoreurology.com You will receive it in word and pdf formats.