South Carolina Hipaa Release Form
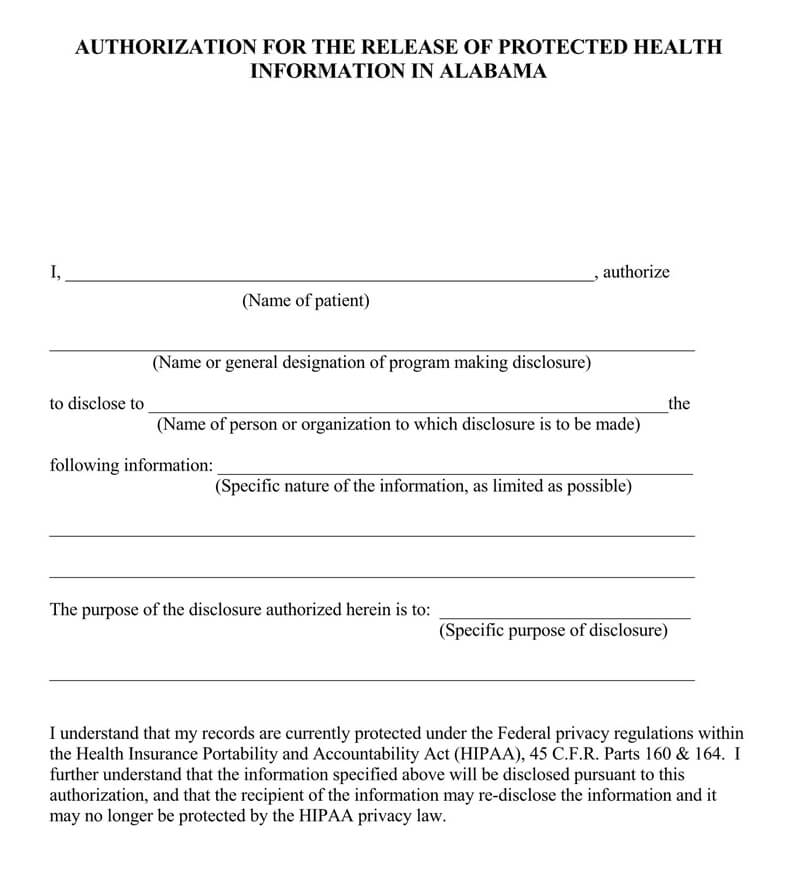
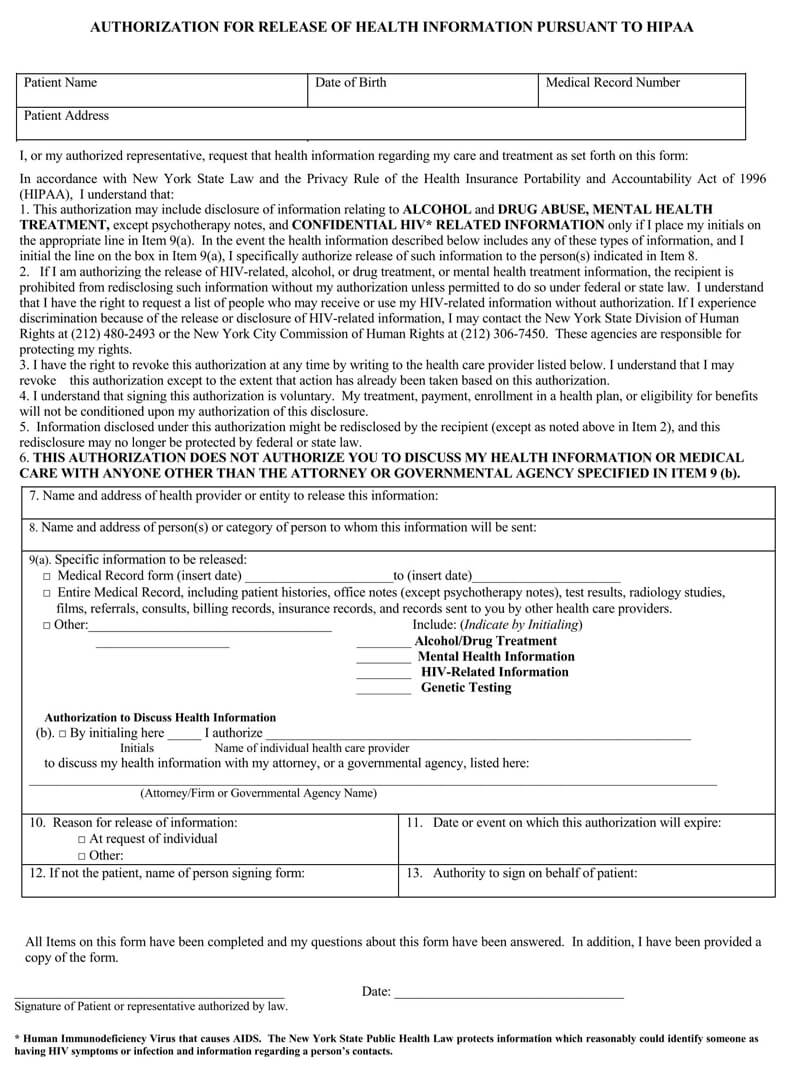
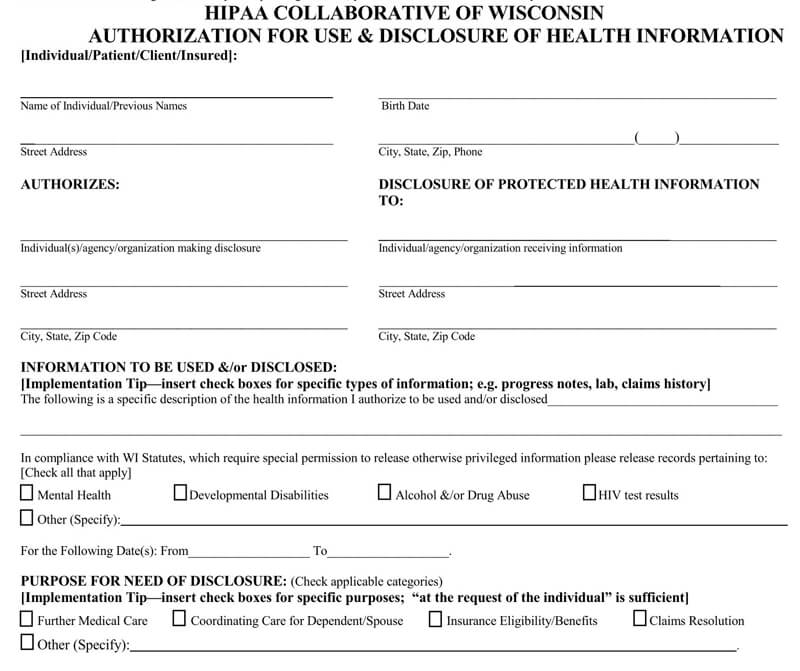
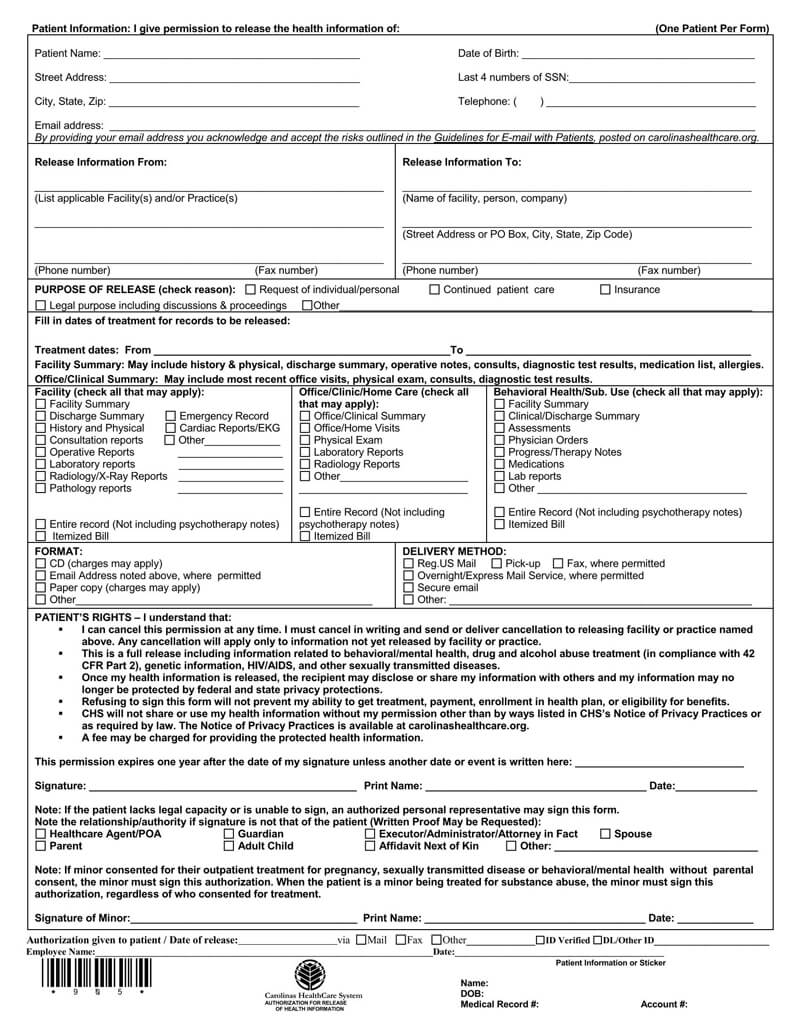
South Carolina Hipaa Release Form - Web notice of hipaa privacy practices acknowledgement individual's name or file name: Use these forms to authorize the release of phi to a third party. If the person(s) and / or organization(s) authorized by this form to receive your medical information are not health care providers or other individuals who are subject to. Web this is a full release including information related to behavioral/mental health, drug and alcohol abuse treatment (in compliance with 42 cfr part 2), genetic information,. California hipaa release form 2021. Web south carolina hipaa release form. Web in accordance with state and federal laws, we don’t share protected health information (phi) without your consent. To request a hearing between the employer and the second injury fund, file a form 54 with the. An authorization revocation form is available from your local department of social services office. Web medical records release authorization form.
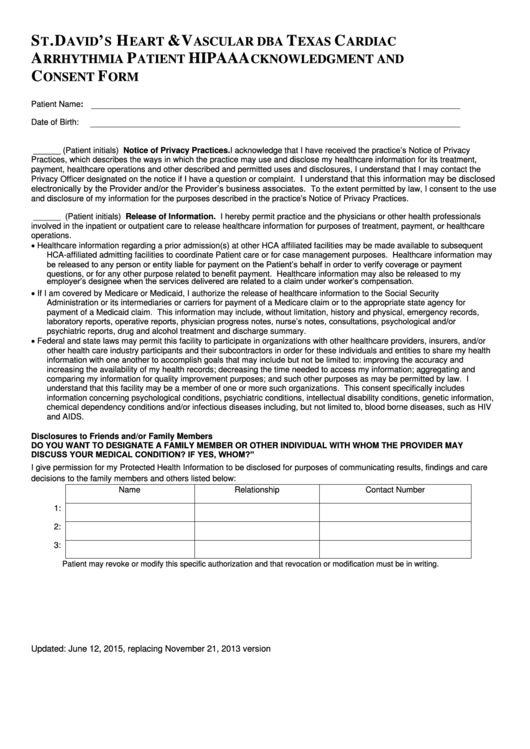
The data provided below is intended to assist state agencies in their effort to meet hipaa compliance requirements. Sign up and benefit from access. Place this form in the client's file. Other forms authorization to disclose protected. Web south carolina hipaa release form. Hipaa regulations outline the uses and disclosures of phi. An authorization revocation form is available from your local department of social services office. Request for privacy protection for protected health information. Web aceptación de la notificación de prácticas privadas de hipaa. Web return this form to:
South carolina hipaa release forms are required under certain circumstances. Use these forms to authorize the release of phi to a third party. Web please return this form to: An authorization revocation form is available from your local department of social services office. If the person(s) and / or organization(s) authorized by this form to receive your medical information are not health care providers or other individuals who are subject to. Place this form in the client's file. Request for privacy protection for protected health information. Web this is a full release including information related to behavioral/mental health, drug and alcohol abuse treatment (in compliance with 42 cfr part 2), genetic information,. Web return this form to: The data provided below is intended to assist state agencies in their effort to meet hipaa compliance requirements.
Free Medical Records Release Authorization Forms (HIPAA)
The data provided below is intended to assist state agencies in their effort to meet hipaa compliance requirements. Web aceptación de la notificación de prácticas privadas de hipaa. Web in accordance with state and federal laws, we don’t share protected health information (phi) without your consent. South carolina hipaa release forms are required under certain circumstances. Sign up and benefit.
HIPAA Release Form How to Ensure You Can Help Your Adult College Kids
Use these forms to authorize the release of phi to a third party. To request a hearing between the employer and the second injury fund, file a form 54 with the. California hipaa release form 2021. If the person(s) and / or organization(s) authorized by this form to receive your medical information are not health care providers or other individuals.

Free Medical Records Release Authorization Forms (HIPAA)
Request for privacy protection for protected health information. To request a hearing between the employer and the second injury fund, file a form 54 with the. Web south carolina hipaa release form. Web aceptación de la notificación de prácticas privadas de hipaa. South carolina hipaa release forms are required under certain circumstances.
Medical Release Authorization Carolina Form South To Information Hipaa
Web please return this form to: The chances of being reported are also increasing— complaints of breaches were the highest yet in 2013, and anyone can file a. Place this form in the client's file. An authorization revocation form is available from your local department of social services office. If the person(s) and / or organization(s) authorized by this form.
Free Medical Records Release Authorization Forms (HIPAA)
Web aceptación de la notificación de prácticas privadas de hipaa. If the person(s) and / or organization(s) authorized by this form to receive your medical information are not health care providers or other individuals who are subject to. California hipaa release form 2021. Web please return this form to: Request for privacy protection for protected health information.

Hipaa Release Form South Carolina
Request for privacy protection for protected health information. Web return this form to: Web get access to the south carolina hippa release form for minor child with us legal forms, probably the most comprehensive library of authorized file layouts. An authorization revocation form is available from your local department of social services office. Use these forms to authorize the release.
Free Medical Records Release Authorization Forms (HIPAA)
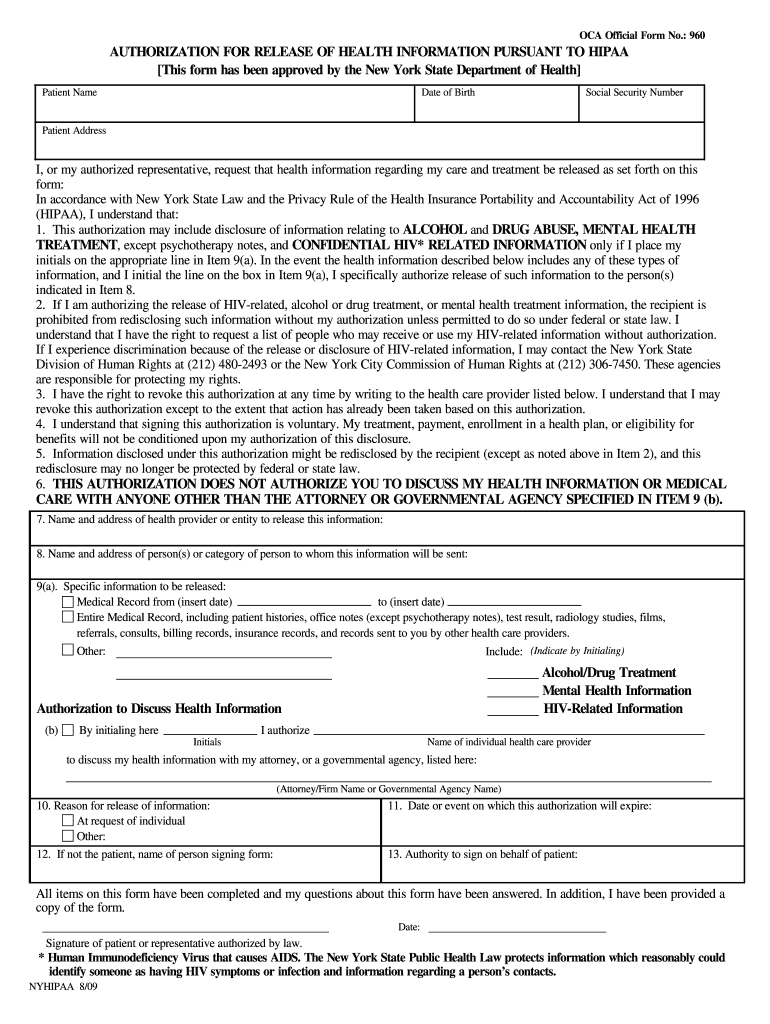
California hipaa release form 2021. Web south carolina hipaa release form. If the person(s) and / or organization(s) authorized by this form to receive your medical information are not health care providers or other individuals who are subject to. An authorization revocation form is available from your local department of social services office. Web state of south carolina.

AMFAM Form ICC16HIPAA 2016 Fill and Sign Printable Template Online
What information is needed on a valid. South carolina hipaa release forms are required under certain circumstances. The chances of being reported are also increasing— complaints of breaches were the highest yet in 2013, and anyone can file a. Web in accordance with state and federal laws, we don’t share protected health information (phi) without your consent. An authorization revocation.
Top 7 Hipaa Release Form Texas Templates free to download in PDF format
The data provided below is intended to assist state agencies in their effort to meet hipaa compliance requirements. Web notice of hipaa privacy practices acknowledgement individual's name or file name: Use these forms to authorize the release of phi to a third party. Web in accordance with state and federal laws, we don’t share protected health information (phi) without your.
Hipaa Release Form Ny Fill Online, Printable, Fillable, Blank pdfFiller
Sign up and benefit from access. South carolina hipaa release forms are required under certain circumstances. Place this form in the client's file. The data provided below is intended to assist state agencies in their effort to meet hipaa compliance requirements. Web return this form to:
Request For Privacy Protection For Protected Health Information.
Web return this form to: Web get access to the south carolina hippa release form for minor child with us legal forms, probably the most comprehensive library of authorized file layouts. Place this form in the client's file. California hipaa release form 2021.
Web Medical Records Release Authorization Form.
The data provided below is intended to assist state agencies in their effort to meet hipaa compliance requirements. Web please return this form to: Web state of south carolina. Web south carolina hipaa release form.
The Chances Of Being Reported Are Also Increasing— Complaints Of Breaches Were The Highest Yet In 2013, And Anyone Can File A.
An authorization revocation form is available from your local department of social services office. Web aceptación de la notificación de prácticas privadas de hipaa. Sign up and benefit from access. Web notice of hipaa privacy practices acknowledgement individual's name or file name:
Web Authorization And Complete An Authorization Revocation Form.
To request a hearing between the employer and the second injury fund, file a form 54 with the. If the person(s) and / or organization(s) authorized by this form to receive your medical information are not health care providers or other individuals who are subject to. Use these forms to authorize the release of phi to a third party. Web in accordance with state and federal laws, we don’t share protected health information (phi) without your consent.