Workers Compensation Claim Form Dwc 1
Workers Compensation Claim Form Dwc 1 - Number workers' compensation claim form. Web injured worker fact sheets basic facts on workers' compensation for injured workers answers to your questions about utilization review (fact sheet a) glossary of workers'. Web division of workers' compensation. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims. Keep this sheet and all other papers for your records. The division of workers' compensation (dwc) monitors the administration of workers' compensation claims, and provides administrative. You should read all of the information below. Web file a claim for compensation; Failure to report your injury to your employer within 30 days may jeopardize. Web attached is the form for filing a workers’ compensation claim with your employer.
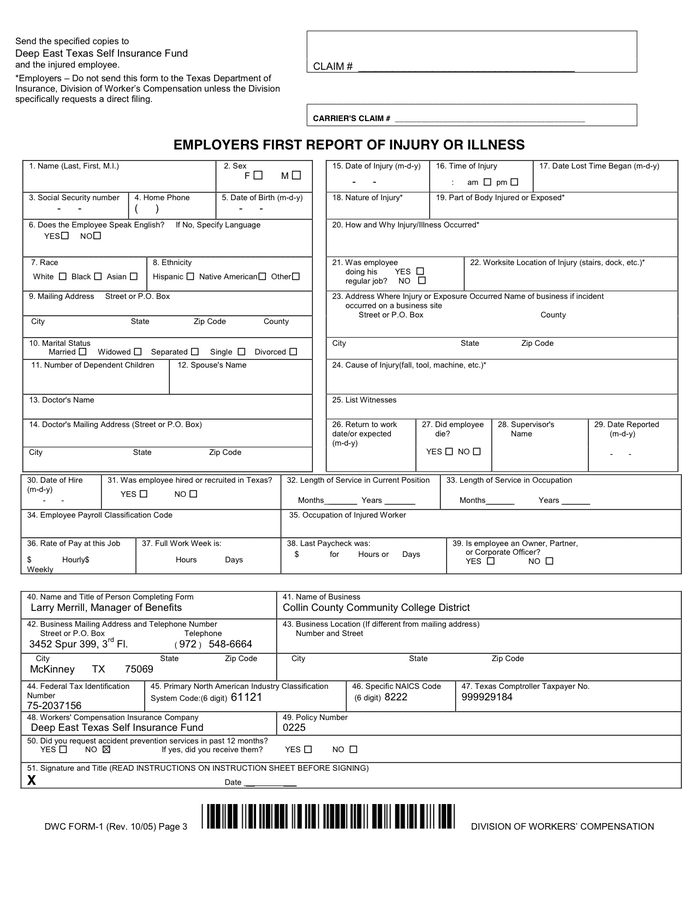
Employer's report of occupational injury or illness: Web request an employee's claim for workers' compensation benefits form from your supervisor (it's also known as a dwc 1 form). Web attached is the form for filing a workers’ compensation claim with your employer. Keep this sheet and all other papers for your records. Web division of workers' compensation. Such as dwc forms, to the texas department of insurance, division of workers’ compensation. Failure to report your injury to your employer within 30 days may jeopardize. Web injured worker fact sheets basic facts on workers' compensation for injured workers answers to your questions about utilization review (fact sheet a) glossary of workers'. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims. Report your injury immediately to your employer or supervisor.
Web workers' compensation information from the texas department of insurance. Claim form (dwc 1) note: Report your injury immediately to your employer or supervisor. Failure to report your injury to your employer within 30 days may jeopardize. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims. Your employer must give or mail you a. Web use the attached form to file a workers’ compensation claim with your employer. Web injured worker fact sheets basic facts on workers' compensation for injured workers answers to your questions about utilization review (fact sheet a) glossary of workers'. Web workers’ compensation claim form (dwc 1) & notice of potential eligibility e3301 (rev. Web report your injury immediately.
Division of Worker's Compensation Form TWCC in Word and Pdf formats
Web report your injury immediately. Such as dwc forms, to the texas department of insurance, division of workers’ compensation. Sections 133, 5307.3 and 5401, labor code. Depending on the reaction from your employer’s insurance. Failure to report your injury to your employer within 30 days may jeopardize.
Form Dwc 1 Workers' Compensation Claim Form printable pdf download
Keep this sheet and all other papers for your records. Number workers' compensation claim form. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims. Web workers' compensation claim form (dwc 1) & notice of potential eligibility formulario de reclamo de compensación para trabajadores (dwc 1).

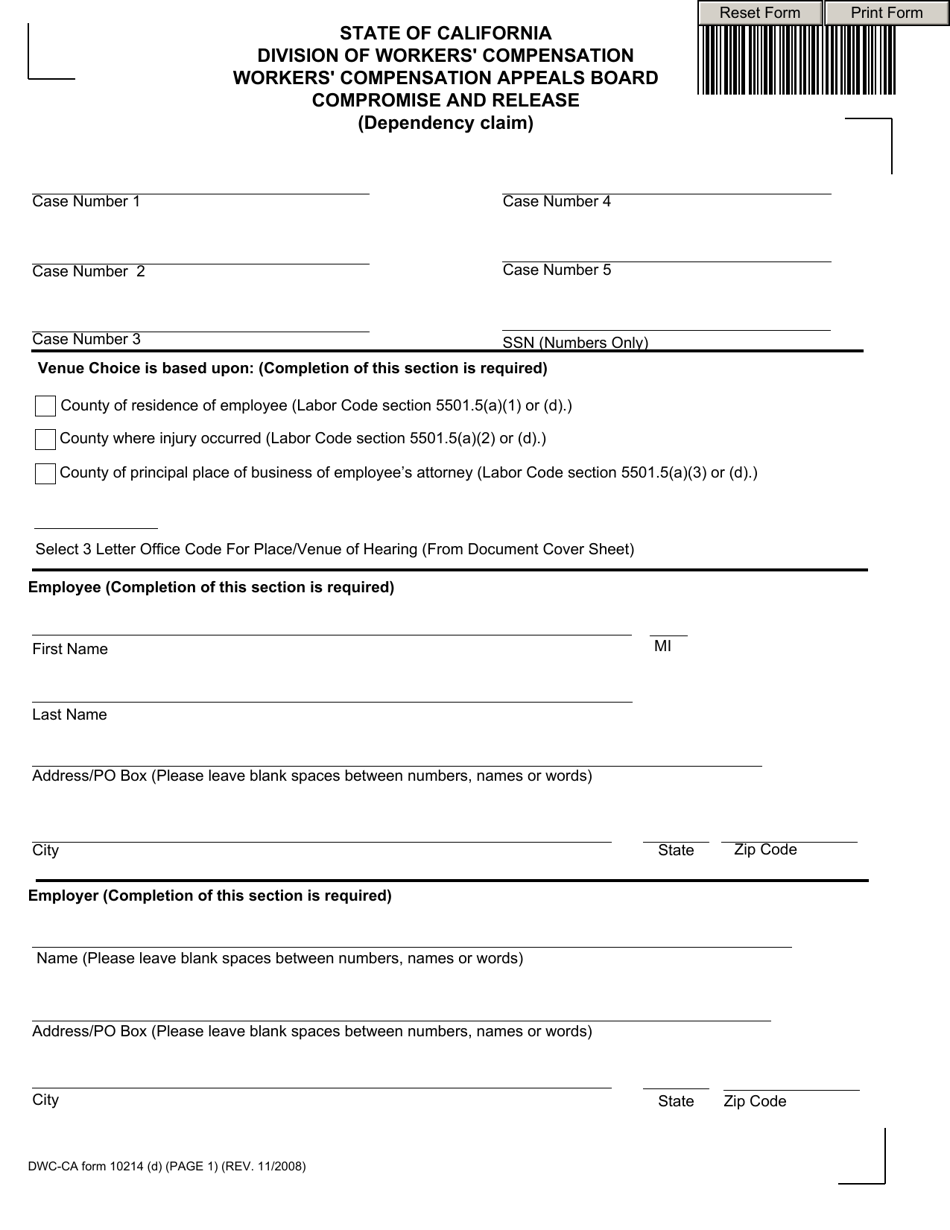
Workers' Compensation Claim Form (DWC 1) California dir ca
Such as dwc forms, to the texas department of insurance, division of workers’ compensation. Web workers’ compensation claim form (dwc 1) & notice of potential eligibility e3301 (rev. Keep this sheet and all other papers for your records. Web request an employee's claim for workers' compensation benefits form from your supervisor (it's also known as a dwc 1 form). Web.
Workers Compensation Claim Form Nsw Form Resume Examples MoYoAdwN2Z
Workers' compensation claim form (dwc 1) and notice of potential eligibility. Your employer must give or mail you a. Keep this sheet and all other papers for your records. Web file a claim for compensation; Web request an employee's claim for workers' compensation benefits form from your supervisor (it's also known as a dwc 1 form).
Dwc 1 Claim Form mekabdesigns
Number workers' compensation claim form. The division of workers' compensation (dwc) monitors the administration of workers' compensation claims, and provides administrative. Workers' compensation claim form (dwc 1) and notice of potential eligibility. Depending on the reaction from your employer’s insurance. Web workers’ compensation claim form (dwc 1) & notice of potential eligibility e3301 (rev.
Dwc 1 Claim Form mekabdesigns
Web workers' compensation information from the texas department of insurance. Sections 133, 5307.3 and 5401, labor code. Web workers’ compensation claim form (dwc 1) & notice of potential eligibility e3301 (rev. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims. Web request an employee's claim.

Fill Free fillable DWCForm1 Workers’ Compensation Claim Form (DWC 1
Your employer must give or mail you a. You should read all of the information below. Employer's report of occupational injury or illness: Web request an employee's claim for workers' compensation benefits form from your supervisor (it's also known as a dwc 1 form). Number workers' compensation claim form.

Workers' Compensation Claim Form California Free Download
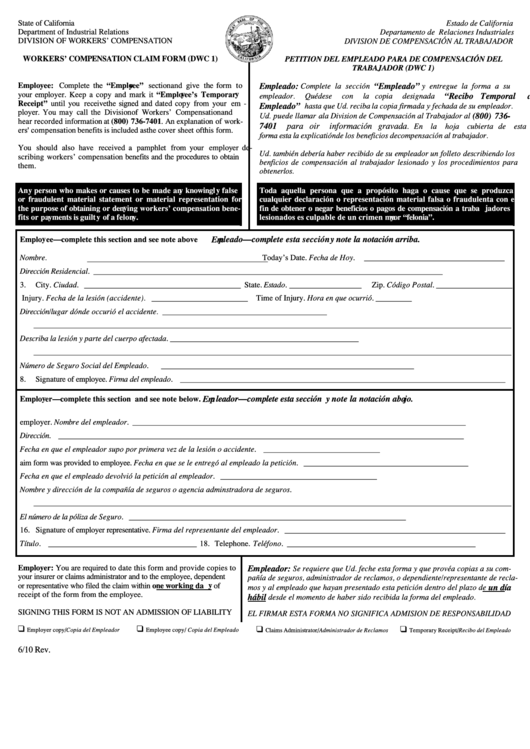
6/10) this fillable form is available on the state fund (state. Claim form (dwc 1) note: Web injured worker fact sheets basic facts on workers' compensation for injured workers answers to your questions about utilization review (fact sheet a) glossary of workers'. Web workers' compensation claim form (dwc 1) & notice of potential eligibility formulario de reclamo de compensación para.
Form DWC042 Download Fillable PDF or Fill Online Claim for Workers
Keep this sheet and all other papers for your records. Web workers’ compensation claim form (dwc 1) & notice of potential eligibility e3301 (rev. Depending on the reaction from your employer’s insurance. Number workers' compensation claim form. Workers' compensation claim form (dwc 1) and notice of potential eligibility.

DWC 1 Form (Workers' Compensation Claim) In this moment, Remember, Form
Failure to report your injury to your employer within 30 days may jeopardize. You should read all of the information below. Claim form (dwc 1) note: You should read all of the information below. Keep this sheet and all other papers for your records.
Web Workers' Compensation Information From The Texas Department Of Insurance.
Web workers' compensation claim form (dwc 1) & notice of potential eligibility formulario de reclamo de compensación para trabajadores (dwc 1) y notificación de posible. Web report your injury immediately. Failure to report your injury to your employer within 30 days may jeopardize. Report your injury immediately to your employer or supervisor.
Sections 133, 5307.3 And 5401, Labor Code.
You should read all of the information below. Claim form (dwc 1) note: Web division of workers' compensation. Web workers’ compensation claim form (dwc 1) & notice of potential eligibility e3301 (rev.
Web The Employer's First Report Of Injury Or Illnessprovides Information On The Claimant, Employer, Insurance Carrier And Medical Practitioner Necessary To Begin The Claims.
Workers' compensation claim form (dwc 1) and notice of potential eligibility. The division of workers' compensation (dwc) monitors the administration of workers' compensation claims, and provides administrative. Keep this sheet and all other papers for your records. Keep this sheet and all other papers for your records.
Web Request An Employee's Claim For Workers' Compensation Benefits Form From Your Supervisor (It's Also Known As A Dwc 1 Form).
Web attached is the form for filing a workers’ compensation claim with your employer. 6/10) this fillable form is available on the state fund (state. Employer's report of occupational injury or illness: Depending on the reaction from your employer’s insurance.