Doh Form Printable
Doh Form Printable - Print your child’s name and birthdate, and sign your name where indicated on page one. Web 20 hours agothe completed forms will be attached to original birth records and provided to adoptees who request their records once they are available next year. Patient identifying information (use additional paper if necessary) 2. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Month day year mobile phone number (patient or guardian): Expanded syringe access program (esap) forms; Adoptee's request for his/her original birth certificate from an adoption sealed file. Web new york state department of health health home consent office of health insurance programs withdrawal of release of educational records instructions: Locate doh form printable and then click get form to get started. Web new york state department of health application for approval of bureau of early intervention individual evaluators,.
Web new york state department of health health home consent office of health insurance programs withdrawal of release of educational records instructions: Web double check all the fillable fields to ensure total precision. Web department of health to get a copy of your child’s cis: Web patients can now log on to our secure server directly and print electronically certified copies of dh form 680 from their home computers, if their healthcare provider is a participating physician and provides them with the state imm id and certification pin of. Web how to change and esign doh downloadable forms version 5 without breaking a sweat. The emergency after hours number will only be in operation after 5:00pm to 8:30am on business days, weekends, and care design ny holidays. To fill out the form by hand: Regardless of the contact preference expressed by birth parents, adopted people will still be eligible to. Web rather, they must use the health home patient information sharing consent form (doh 5055)]. Web new york state department of health application for approval of bureau of early intervention individual evaluators,.
The third indictment against former president donald trump was released tuesday. Instructions for parent/guardian/legally authorized representative:. Information about patient (please print) name: Print or type name title individual acknowledgment state of new york ) county of ) ss.: Regardless of the contact preference expressed by birth parents, adopted people will still be eligible to. This form is to withdraw (take away) consent (permission) to release educational records (which. The emergency after hours number will only be in operation after 5:00pm to 8:30am on business days, weekends, and care design ny holidays. Americans with disabilities act complaint form (pdf) asbestos. Utilize a check mark to point the choice where required. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form.
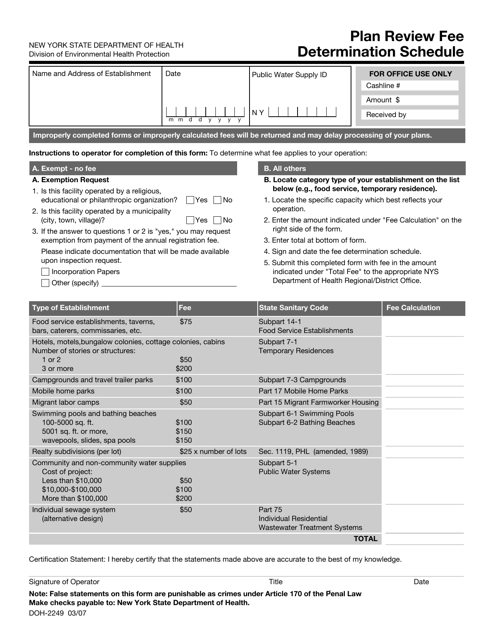
Form DOH2249 Download Printable PDF or Fill Online Plan Review Fee
Americans with disabilities act complaint form (pdf) asbestos. Web 20 hours agothe completed forms will be attached to original birth records and provided to adoptees who request their records once they are available next year. Hiv/aids educational materials order forms; Forms are available in electronic format only (word or pdf). A grand jury indicted trump for a raft of alleged.
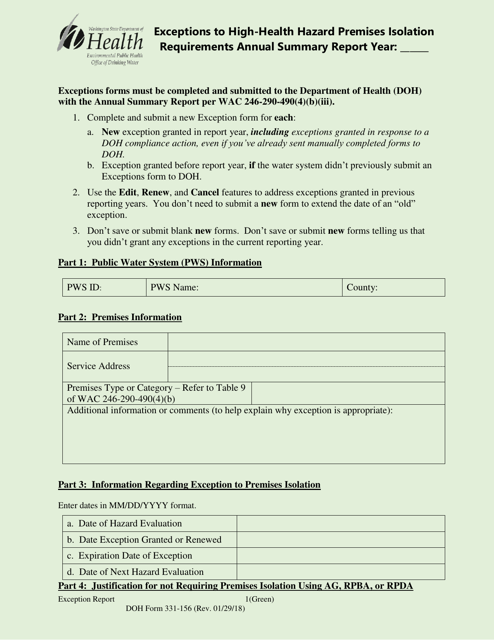
DOH Form 331156 Download Printable PDF or Fill Online Exceptions to
Patient identifying information (use additional paper if necessary) 2. Web these forms are for ordering tests and supplies from the public health laboratories. The emergency after hours number will only be in operation after 5:00pm to 8:30am on business days, weekends, and care design ny holidays. Web required hiv related consent & authorization forms; (last, first, middle) case number:

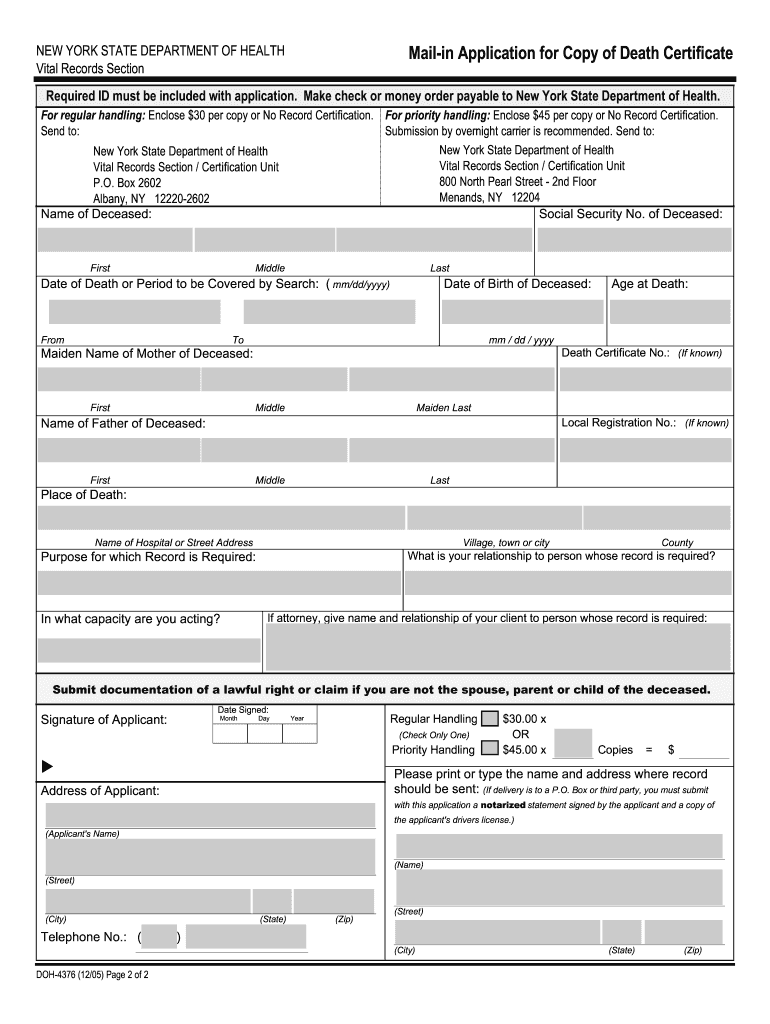
Form DOH4316 Download Printable PDF or Fill Online Assignment of
Locate doh form printable and then click get form to get started. Web 20 hours agothe completed forms will be attached to original birth records and provided to adoptees who request their records once they are available next year. To fill out the form by hand: Web 13 hours agoby washington post staff. Utilize a check mark to point the.
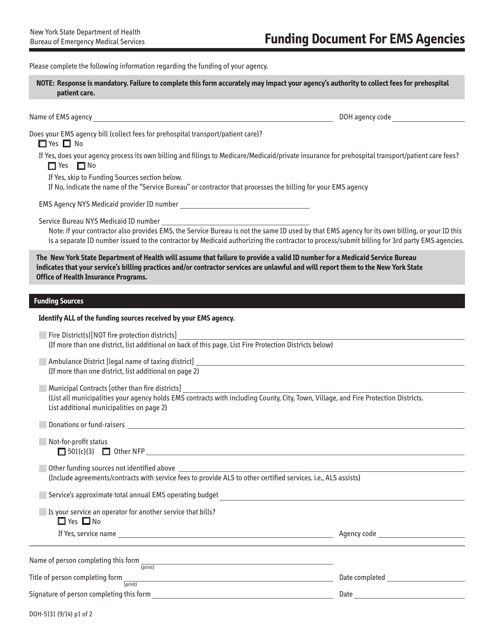
Form DOH5131 Download Fillable PDF or Fill Online Funding Document for
Patient identifying information (use additional paper if necessary) 2. Web required hiv related consent & authorization forms; Americans with disabilities act complaint form (pdf) asbestos. If you have questions concerning a form, contact your regional office. Web rather, they must use the health home patient information sharing consent form (doh 5055)].

Doh 4359 Fill Online, Printable, Fillable, Blank pdfFiller
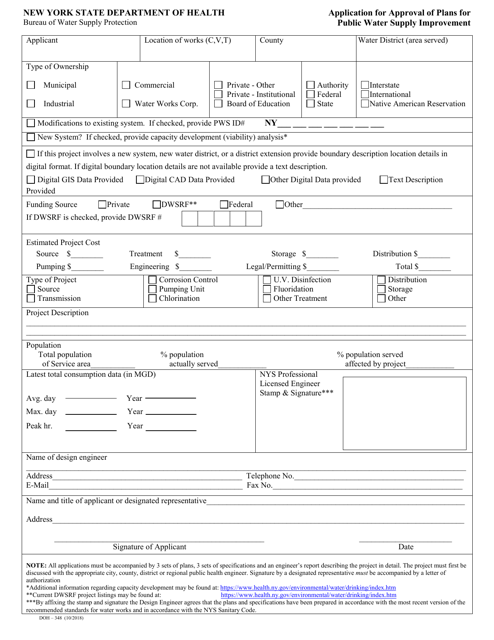
Web new york state department of health application for approval of bureau of early intervention individual evaluators,. Adoptee's request for his/her original birth certificate from an adoption sealed file. Forms are available in electronic format only (word or pdf). Web new york state department of health health home consent office of health insurance programs withdrawal of release of educational records.
Doh Form Fill Out and Sign Printable PDF Template signNow
Hiv/aids educational materials order forms; Make use of the sign tool to create and add your electronic signature to signnow the doh 2094 form. Web department of health to get a copy of your child’s cis: Utilize a check mark to point the choice where required. Press done after you complete the document.
Form DOH348 Download Printable PDF or Fill Online Application for
Print your child’s name and birthdate, and sign your name where indicated on page one. Web patients can now log on to our secure server directly and print electronically certified copies of dh form 680 from their home computers, if their healthcare provider is a participating physician and provides them with the state imm id and certification pin of. Web.
Doh Form Fill Out and Sign Printable PDF Template signNow
Regardless of the contact preference expressed by birth parents, adopted people will still be eligible to. Forms are available in electronic format only (word or pdf). Instructions for parent/guardian/legally authorized representative:. Web rather, they must use the health home patient information sharing consent form (doh 5055)]. Download the forms in pdf, and then fill them out following instructions.
Doh Application Form for Renewal of License to Operate Fill Out and
Highlight relevant paragraphs of your documents or. Adoptee's request for his/her original birth certificate from an adoption sealed file. Web rather, they must use the health home patient information sharing consent form (doh 5055)]. Print name of health home print name of child child’s date of birth section 1: Web required hiv related consent & authorization forms;
Doh Waiver Forms Fill Online, Printable, Fillable, Blank PDFfiller
Make use of the sign tool to create and add your electronic signature to signnow the doh 2094 form. Utilize a check mark to point the choice where required. This form is to withdraw (take away) consent (permission) to release educational records (which. Web new york state department of health health home consent office of health insurance programs withdrawal of.
Web These Forms Are For Ordering Tests And Supplies From The Public Health Laboratories.
August 1, 2023 at 5:45 p.m. Covid19 sample submission (pdf) public health laboratories specimen. Web required hiv related consent & authorization forms; (last, first, middle) case number:
Web Need A Blank Doh Form?
Now you can print, download, or. Web new york state department of health health home consent office of health insurance programs withdrawal of release of educational records instructions: Download the forms in pdf, and then fill them out following instructions. Highlight relevant paragraphs of your documents or.
Make Use Of The Tools We Offer To Fill Out Your Document.
Press done after you complete the document. Web patients can now log on to our secure server directly and print electronically certified copies of dh form 680 from their home computers, if their healthcare provider is a participating physician and provides them with the state imm id and certification pin of. Patient identifying information (use additional paper if necessary) 2. Information about patient (please print) name:
Utilize A Check Mark To Point The Choice Where Required.
Month day year mobile phone number (patient or guardian): Make use of the sign tool to create and add your electronic signature to signnow the doh 2094 form. Write the date of each vaccine dose. Adoptee's request for his/her original birth certificate from an adoption sealed file.