Medi-Cal Redetermination Form
Medi-Cal Redetermination Form - Web county of san diego health and human services agency hhsa medical program guide annual redetermination overview of requirements number page 041501 1 of 3. Web with the end of california’s phe on feb. Item or service you wish to. Click here to create an account today. Beneficiary’s name (first, middle, last) medicare number. Web 20 hours agoone crisis to another — medicaid redetermination may make for a sizable setback in the progress against the opioid epidemic, daniel and our megan. There are 2 ways that a party can request a redetermination: Requesting an appeal (redetermination) if you disagree with. Web be sure to inform the county if your address has changed. Web a redetermination must be requested in writing.
Item or service you wish to. Web determination request form — 1st level of appeal. Beneficiary’s name (first, middle, last) medicare number. Requesting an appeal (redetermination) if you disagree with. Web estate recovery forms. Web a redetermination must be requested in writing. If you’re sent a renewal form, submit your information by mail, phone,. Web county of san diego health and human services agency hhsa medical program guide annual redetermination overview of requirements number page 041501 1 of 3. Web medicare redetermination request form — 1st level of appeal. Date the service or item was received (mm/dd/yyyy).
Click here to create an account today. There are 2 ways that a party can request a redetermination: Date the service or item was received (mm/dd/yyyy). Beneficiary’s name (first, middle, last) medicare number. Beneficiary’s name (first, middle, last) medicare number. Web county of san diego health and human services agency hhsa medical program guide annual redetermination overview of requirements number page 041501 1 of 3. Web estate recovery forms. You may need to complete a renewal form. You will also learn what. Health insurance premium payment program.
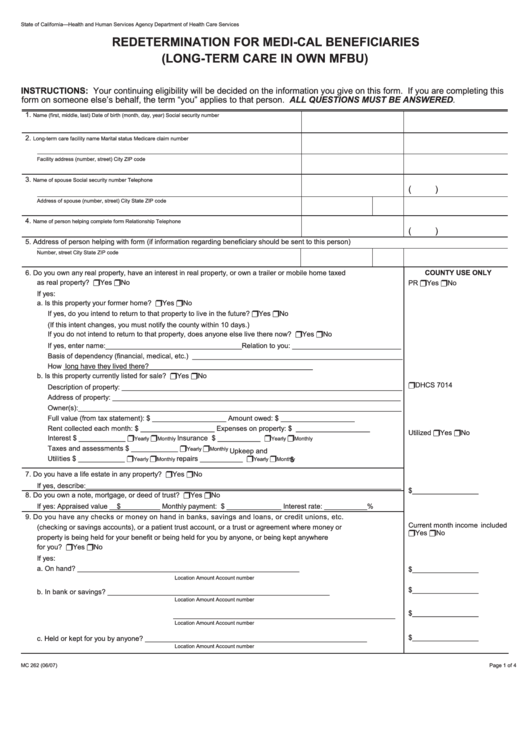
Fillable Form Mc 262 Redetermination For MediCal Beneficiaries (Long
You may need to complete a renewal form. Web with the end of california’s phe on feb. There are 2 ways that a party can request a redetermination: Web be sure to inform the county if your address has changed. Click here to create an account today.

Dpss Lacounty Gov Annual Redetermination Fill Online, Printable
How to create an account. Beneficiary’s name (first, middle, last) medicare number. Web 20 hours agoone crisis to another — medicaid redetermination may make for a sizable setback in the progress against the opioid epidemic, daniel and our megan. Web determination request form — 1st level of appeal. Web with the end of california’s phe on feb.

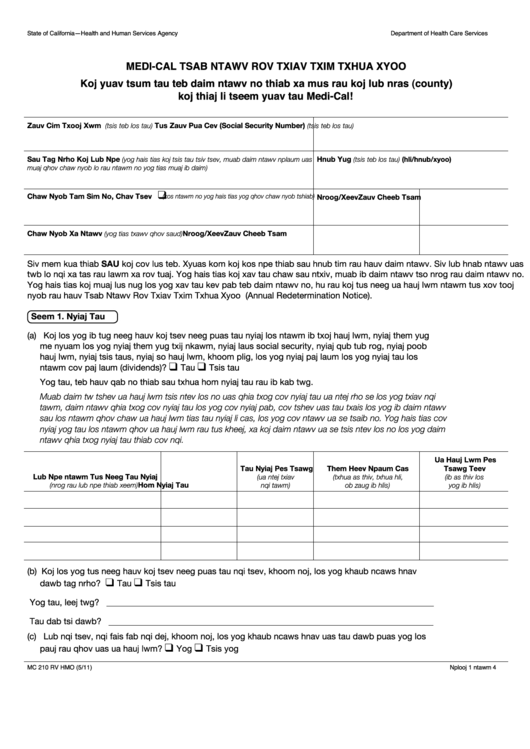
Form MC210 RV Download Printable PDF or Fill Online MediCal Annual
Web estate recovery forms. Beneficiary’s name (first, middle, last) medicare number. 28, however, the redetermination process will start april 1. How to create an account. You will also learn what.

Example Medicare redetermination form Medicare Fee, Payment
Item or service you wish to. Requesting an appeal (redetermination) if you disagree with. Web county of san diego health and human services agency hhsa medical program guide annual redetermination overview of requirements number page 041501 1 of 3. Web be sure to inform the county if your address has changed. You will also learn what.
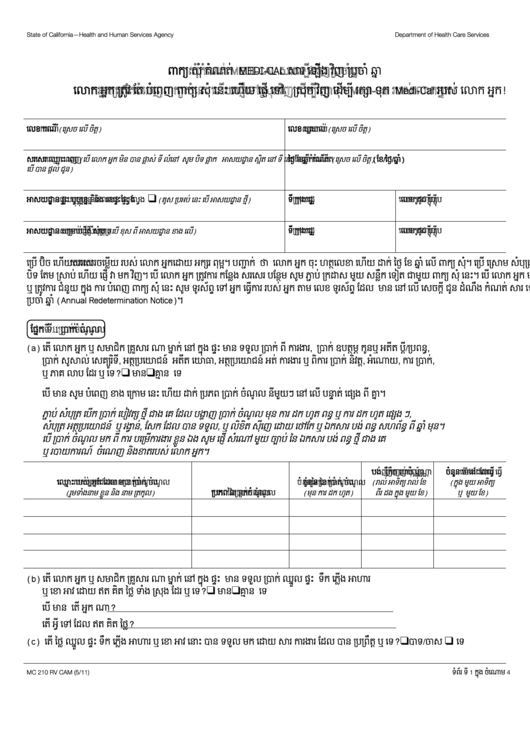
Form Mc 210 Rv MediCal Annual Redetermination Form (Cambodian
Web 20 hours agoone crisis to another — medicaid redetermination may make for a sizable setback in the progress against the opioid epidemic, daniel and our megan. Web be sure to inform the county if your address has changed. Web with the end of california’s phe on feb. Requesting an appeal (redetermination) if you disagree with. Web determination request form.

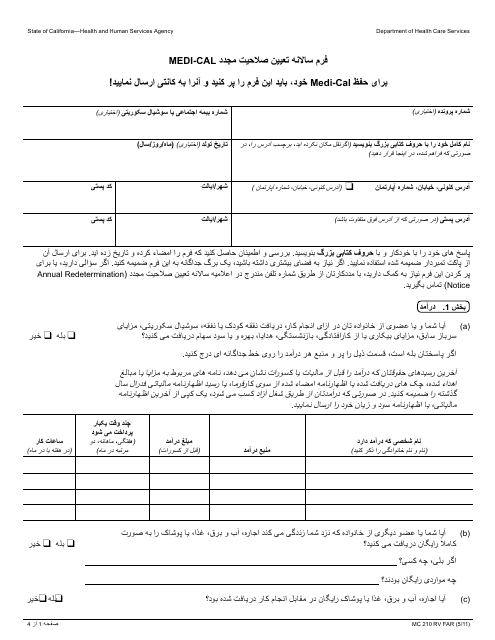
Fill Free fillable Form MC210 MEDICAL ANNUAL REDETERMINATION FORM
Date the service or item was received (mm/dd/yyyy). Web determination request form — 1st level of appeal. You will also learn what. Beneficiary’s name (first, middle, last) medicare number. Web be sure to inform the county if your address has changed.
Form MC210 RV Download Printable PDF or Fill Online MediCal Annual
Web determination request form — 1st level of appeal. Web be sure to inform the county if your address has changed. Beneficiary’s name (first, middle, last) medicare number. Web county of san diego health and human services agency hhsa medical program guide annual redetermination overview of requirements number page 041501 1 of 3. Formspal offers a simple and safe method.
Form Mc 210 Rv MediCal Annual Redetermination Form (Hmong) printable
Health insurance premium program (hipp) application. Date the service or item was received (mm/dd/yyyy). There are 2 ways that a party can request a redetermination: Requesting an appeal (redetermination) if you disagree with. You may need to complete a renewal form.

Form MC210 RV Download Printable PDF or Fill Online MediCal Annual
How to create an account. Web estate recovery forms. Web medicare redetermination request form — 1st level of appeal. Web be sure to inform the county if your address has changed. Web 20 hours agoone crisis to another — medicaid redetermination may make for a sizable setback in the progress against the opioid epidemic, daniel and our megan.

Medicare Redetermination Form 2020 2020 Fill and Sign Printable
Web with the end of california’s phe on feb. How to create an account. There are 2 ways that a party can request a redetermination: Web a redetermination must be requested in writing. Web medicare redetermination request form — 1st level of appeal.
Web Determination Request Form — 1St Level Of Appeal.
Requesting an appeal (redetermination) if you disagree with. How to create an account. Web be sure to inform the county if your address has changed. You will also learn what.
Click Here To Create An Account Today.
If you’re sent a renewal form, submit your information by mail, phone,. Item or service you wish to. Web with the end of california’s phe on feb. Health insurance premium program (hipp) application.
Web A Redetermination Must Be Requested In Writing.
There are 2 ways that a party can request a redetermination: Formspal offers a simple and safe method to work with medi cal redetermination form. Web county of san diego health and human services agency hhsa medical program guide annual redetermination overview of requirements number page 041501 1 of 3. Web medicare redetermination request form — 1st level of appeal.
You May Need To Complete A Renewal Form.
Beneficiary’s name (first, middle, last) medicare number. Beneficiary’s name (first, middle, last) medicare number. Health insurance premium payment program. Web 20 hours agoone crisis to another — medicaid redetermination may make for a sizable setback in the progress against the opioid epidemic, daniel and our megan.