Oregon Form 801
Oregon Form 801 - Web if the county is producing a voters’ pamphlet an explanatory statement must be drafted and attached to this form for: Or any initiative or referendum, if required by local ordinance. Email 801 forms to saif801@saif.com mail completed forms to: Form 801 english — report of job injury or illness. If a form is not listed, it may be included on the publications page. If you do not intend to file a workers’ compensation claim with saif, do not sign the signature line. Web use this form to help you investigate workplace accidents or incidents. It is your right to file a workers’ compensation claim. Signature gathering firm registration (online form) sel 305 : Otherwise, you may be able to just complete a supervisor's accident/incident report form.
Saif corporation, 400 high st se, salem, or 97312 or fax to these numbers: Web complete form 801, “report of job injury or illness,” available from your employer and form 827, “worker’s and health care provider’s report for workers’ compensation claims,” available from your health care provider. You may receive medical treatment from the health care provider of your choice , including: Web you’re in the right place. Yes no authorized county officialnot required to be notarized. No one else should make these decisions for you. Email 801 forms to saif801@saif.com mail completed forms to: Your employer will give you a copy. Web fill out form 801 “report of job injury or illness” and turn it in to your employer. Employer at time of injury complete the rest of this form and give a copy of the form to the worker.
Sb 801 senate committee on labor and business. You also have the right to not file a claim. Form 827 spanish — reporte del trabajador y del proveedor medico para reclamaciones de compensation para trabajadores. All forms are searchable below by form number, title, description, revision date, category, and related bulletins. You must also post the osha 300a where employees can see it, no later than feb. This will let you fill out this form. Web form 801, “report of job injury or illness,” upon your request, or when the employer has notice or knowledge of an injury or exposure. Employer at time of injury complete the rest of this form and give a copy of the form to the worker. Your employer should provide you this form. Contact the sdao workers’ compensation department at 800.

2010 Form SAIF X801 Fill Online, Printable, Fillable, Blank pdfFiller
Web tell your employer right away about your injury and ask for an oregon form 801, the worker’s and employer’s report of occupational injury or disease/illness. Termination of circulator authorization (online form) sel 307 : Web you’re in the right place. Form 801 spanish — reporte de lesión o enfermedad en el trabajo (801s) form 827 english — workers’ and.

Form 2554 Download Printable PDF or Fill Online Employment Search
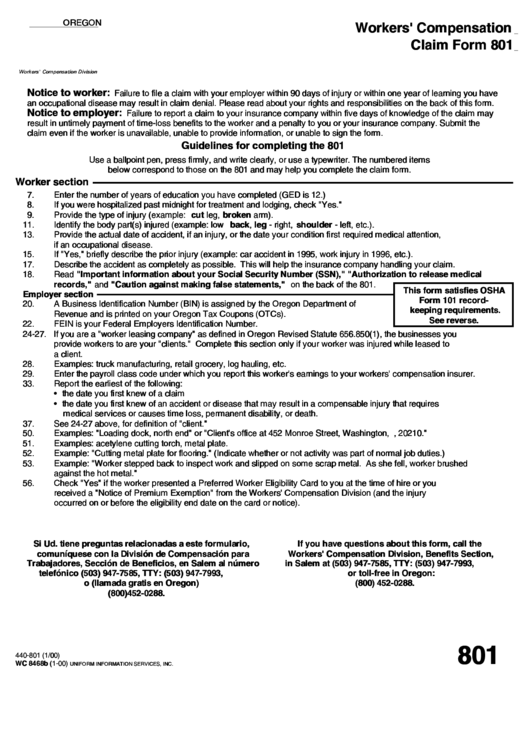
Web workers' compensation claim form 801 form 801 is required to be filled out by the employee when medical treatment is sought for the injured employee. Web saif 801 form for employee injuries where medical attention is sought, the saif 801 form would be completed within 24 hours by the employee and supervisor (utilizing the manager/supervisor instructions for 801 below).
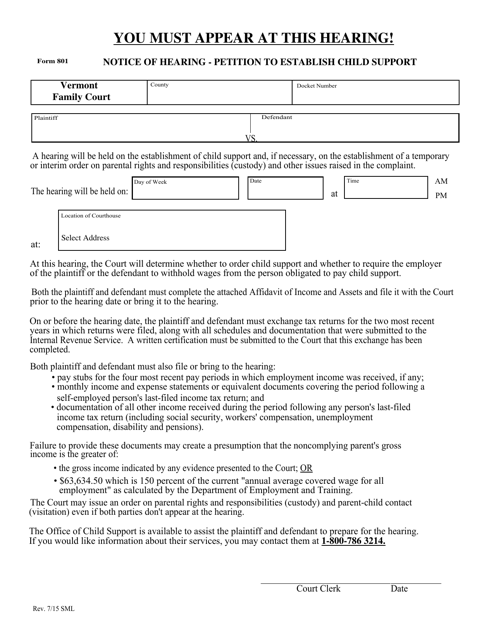
Form 801 Download Fillable PDF or Fill Online Notice of Hearing
You must also post the osha 300a where employees can see it, no later than feb. Summarize that information each year on a form called the osha 300a. All forms are searchable below by form number, title, description, revision date, category, and related bulletins. You may receive medical treatment from the health care provider of your choice , including: It.
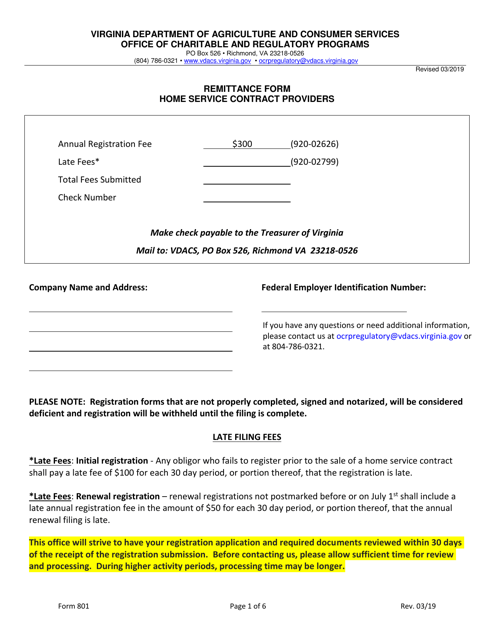
Form 801 Download Fillable PDF or Fill Online Home Service Contract
Web if the county is producing a voters’ pamphlet an explanatory statement must be drafted and attached to this form for: Your employer will give you a copy. No one else should make these decisions for you. If a form is not listed, it may be included on the publications page. You may receive medical treatment from the health care.

2012 OR Form 827 Fill Online, Printable, Fillable, Blank pdfFiller
Or any initiative or referendum, if required by local ordinance. Web workers' compensation claim form 801 form 801 is required to be filled out by the employee when medical treatment is sought for the injured employee. This form is for use within your company. Form 801 spanish — reporte de lesión o enfermedad en el trabajo (801s) form 827 english.

Oregon Form 801 ≡ Fill Out Printable PDF Forms Online
Web tell your employer right away about your injury and ask for an oregon form 801, the worker’s and employer’s report of occupational injury or disease/illness. How do i get medical treatment? Date of injury or illness: Please read about your rights and responsibilities on the back of this form. If you do not intend to file a workers’ compensation.
Form 801 Oregon Workers' Compensation printable pdf download
Your employer should send it to its workers’ compensation insurance carrier within five days of your notice. Your employer will give you a copy. Yes no authorized county officialnot required to be notarized. Please read about your rights and responsibilities on the back of this form. Web form 801 is required by the oregon administrative rules to be completed, signed.

Oregon Pacific Railroad 801
Web workers' compensationclaim form 801 failure to file a claim with your employer within 90 days of injury or within one year of learning you have an occupational disease may result in claim denial. Web fill out form 801 “report of job injury or illness” and turn it in to your employer. Employer at time of injury complete the rest.
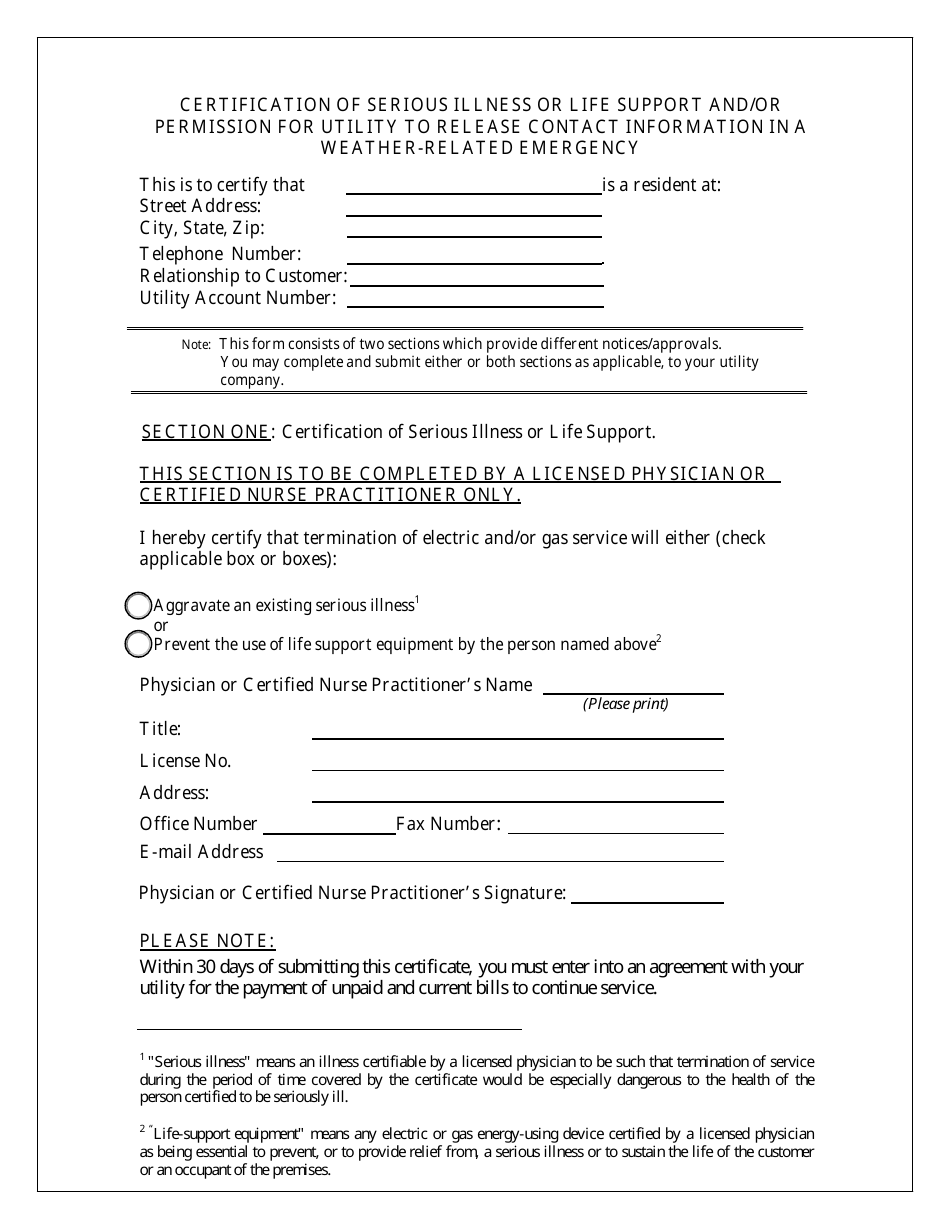
Form PSC801 Download Fillable PDF or Fill Online Certification of
Signature gathering firm registration (online form) sel 305 : Web form 801 is required by the oregon administrative rules to be completed, signed by the employee and the employer, and sent to sdao within five days of the date of injury. Date of injury or illness: Your employer should send it to its workers’ compensation insurance carrier within five days.

Oregon Form Wr 2017 Fill Online, Printable, Fillable, Blank pdfFiller
The ombuds office for oregon workers is the state office that serves as an independent advocate for workers by helping them understand their rights, benefits, protections, and responsibilities within the workers’ compensation system and workplace safety and health laws and rules. Web form 801, “report of job injury or illness,” upon your request, or when the employer has notice or.
Saif Corporation, 400 High St Se, Salem, Or 97312 Or Fax To These Numbers:
If you do not intend to file a workers’ compensation claim with the insurance company, do not sign the signature line. Or any initiative or referendum, if required by local ordinance. It is not intended to replace dcbs form 801: Your employer will give you a copy.
Your Employer Should Send It To Its Workers’ Compensation Insurance Carrier Within Five Days Of Your Notice.
Your employer should provide you this form. Web fill out form 801 “report of job injury or illness” and turn it in to your employer. Web complete form 801, “report of job injury or illness,” available from your employer and form 827, “worker’s and health care provider’s report for workers’ compensation claims,” available from your health care provider. Show details how it works upload the oregon workers compensation form 801 edit & sign 801 form workers compensation oregon from anywhere save your changes and share 801 form
Any Measure Referred By The County Governing Body;
You must also post the osha 300a where employees can see it, no later than feb. Sb 801 senate committee on labor and business. Web saif 801 form for employee injuries where medical attention is sought, the saif 801 form would be completed within 24 hours by the employee and supervisor (utilizing the manager/supervisor instructions for 801 below) and returned to heidi melton in insurance and risk management services. Oregon state legislature building hours:
Yes No Authorized County Officialnot Required To Be Notarized.
The ombuds office for oregon workers is the state office that serves as an independent advocate for workers by helping them understand their rights, benefits, protections, and responsibilities within the workers’ compensation system and workplace safety and health laws and rules. This form is for use within your company. Employer at time of injury complete the rest of this form and give a copy of the form to the worker. Termination of circulator authorization (online form) sel 307 :